Chapter 8
Planning ratio, allocations and funding of community care and high- and low-care
He who would pass his declining years with honor and comfort,
should, when young, consider that he may one day become old, and remember when
he is old, that he has once been young.
Joseph Addison 1672 – 1719
Introduction
8.1
This chapter considers whether the current planning ratio between community,
high- and low-care places is appropriate. It also addresses the impact of
current and future residential places allocation and funding on the number and
provision of community care places.
Current planning ratio
8.2
The current planning ratio of 113 places per 1000 people aged 70 years and
over is allocated as follows:
-
44 high care places per 1000
people aged 70 years and over;
-
44 low care places per 1000 people
aged 70 years and over;
-
25 (21 CACP and 4 EACH) community
care places per 1000 people aged 70 years and over.[1]
8.3
The process of allocating new places begins with an estimation of the
number of new places needed to meet increases in the target population. Aged
Care Planning Advisory Committees in each state and territory then consider how
new places should be distributed between regions and special needs groups and
advise the Secretary of the Department of Health and Ageing (the department) on
the most appropriate allocation and distribution by different types of subsidy
and proportions of care. Under the 2008–09 Aged Care Approvals Round (ACAR), 10
447 aged care places were allocated of which 73 per cent were residential places.[2]
8.4
The Aged Care Act 1997 specifies the objectives of the planning
process:
-
to provide and open and clear
planning process; and
-
to identify community needs,
particularly in respect of people with special needs; and
-
to allocate places in a way that best
meets the identified needs of the community.[3]
8.5
Persons with special needs are defined by the Aged Care Act 1997
as:
-
people from Aboriginal and Torres
Strait Islander communities;
-
people from non-English speaking
backgrounds;
-
people who live in rural and
remote areas;
-
people who are financially or
socially disadvantaged;
-
people of a kind (if any)
specified in the Allocation Principles.[4]
8.6
Of the planning system, the Department of Health and Ageing commented
that:
The planning framework ensures that the growth in the number
of aged care places matches growth in the aged population. It also ensure
balance in the provision of services between metropolitan, regional, rural and
remote areas.[5]
Issues with the current planning system
8.7
Providers raised a range of concerns in relation to the current planning
system. Amongst them, the Aged Care Association Australia (ACAA) stated that
the current system is:
...very inappropriate in meeting these objectives as the ratio
is not delivering a well planned and coordinated balance between demand and
supply.[6]
8.8
A major concern highlighted by a number of providers was that the
current planning system did not recognise the growth in residents in high care.
ACCA, for example, noted:
There appears to be little or no science to the increases in
the formula and only appear to be intended for one purpose namely, increasing
the number of community care places. The 2008 Report on the Operation of the
Aged Care Act 1997, shows that forty five percent of residents in low care
facilities are actually high care classified and that sixty nine percent of all
aged care residents are classified as high care.[7]
8.9
The Australian Institute of Health and Welfare (AIHW) held that it was
timely to review the planning ratio, noting that whilst there has been a steady
rise in the number of permanent residents classified as high care including 70
per cent in 2007, only 49 per cent of places were designated as high care in
2007.[8]
At the same time, the AIHW cited the 2008 Report on Government Services which highlighted
that by 30 June 2007, 37 per cent of low care places were occupied by residents
with high care needs whilst 67 per cent of all operational places were taken up
by high care residents.[9]
8.10
Similarly, the Aged Care Association Australia – SA Inc held that the
current planning ratio is not appropriate as the residential aged care
population comprises 70 per cent high care residents. According to the
association, there exists a 'vast disconnect' between the actual residential
care population and the planning ratio between residential high and low care.[10]
Moreover, the association argued that as the proportion of high care residents
is bound to increase over time, the current ratio will become increasingly
inappropriate.
8.11
Mr Alan Gruner of The Brotherhood of St Laurance also commented:
The ratio, in terms of residential care, is fifty-fifty
between high care and low care. In our opinion, there should be a higher ratio
of high care—at least a 70 to 30 ratio—given the needs of people coming into
residential care and particularly the higher health care they need.[11]
8.12
Mr Gruner went on to state that the future with residential care 'is
very much towards the high end, not just because of the ACFI but because of the
needs of people as they age'. He noted that many clients requiring low care use
community care packages, where they can access those packages and 'that seems
more appropriate'.[12]
8.13
However, Mr Andrew Stuart, First Assistant Secretary of the Department
of Health and Ageing responded to such concerns:
Half of all residents entering care for the first time enter
at low care, but about 70 per cent of all residents in care at any point in
time are in high care. We think those two pieces of information are actually
quite separate considerations. The first one is about access and wanting to
make sure that people at both low-care and high-care levels can access aged
care appropriately. The second is about ageing in place. Once people are in
care they are able to stay in their current place and age in place within the
service.[13]
8.14
Problems with occupancy rates due to the planning system were also
raised in relation to the consideration of state-wide rather than local
demographic information. The House Group of Companies as one case in point
noted that their facilities have experienced vacancy rates of up to 94 per cent
due to 'flawed planning ratios which allowed more than six new services to
commence operation within a short distance from the Gleneagles, in
north-eastern Adelaide'. According to the group, in some areas there are
serious shortfalls in place, whilst in others, there has been an over-supply.[14]
8.15
Aged and Community Services Australia (ACSA) held the same view:
Currently little account is taken of services not directly
funded by the Australian Government, allocations are made on the basis of quite
large planning regions which sometimes mask the needs of specific communities
and it would be appropriate to test the effect of introducing a weighting for
the number of very old people (85+) in an area.[15]
8.16
Mr Greg Mansour of Aged and Community Care Victoria also commented that the
planning region model of planning leads to misallocations:
So what happens is the beds are allocated within a planning
region. The planning region boundary does not necessarily reflect the community
boundary, and you could have nearby towns where the boundary runs between those
towns...
Yes, I hear that feedback and I also hear it probably even
stronger in relation to community aged-care packages. It is not uncommon for
some of our members in certain geographic areas to have vacancies on one side
of the boundary and waiting lists on the other. So whilst the regional
boundaries are probably—and I can understand why they are important from a
planning point of view, but if they are inflexible and they do not operate
seamlessly, it will create a problem for communities and I get that feedback.[16]
8.17
Mr Mansour went on to argue that the planning system needs to allow
consumer choice so that the appropriate packages can be offered. However, Mr
Mansour contended that although this is critically important, there are a range
of barriers. For example, if a particular community had a high level of
interest in community care there is not a simple straightforward process to
allow for the swapping of low-care beds to community aged-care packages. Mr
Mansour concluded that 'there is a whole lot of systems that we have put in
place, I guess, as checks and balances that inhibit flexibility'.[17]
8.18
The relationship between planning ratios and occupancy rates and their
impact on the viability of aged care providers was highlighted by a number of
witnesses including the Royal College of Nursing, Australia which
stated:
Planning for distribution of approved residential and
community aged care places requires more strategic targeting with greater
attention given to maintaining a comprehensive service able to meet different
levels of resident needs. The low level of funding provided for occupied beds
means that aged care organisations rely heavily on high occupancy rates to be
sustainable.[18]
8.19
The ACAA estimated that the average occupancy in the industry has
significantly declined. Utilising June 2007 occupancy levels, the ACAA
maintained that the average occupancy has fallen to 93 per cent as at 30 June
2008.[19]
Indeed, the Report on the Operation of the Aged Care Act 1997 for 2008
stated of the occupancy rate in residential care:
At 30 June 2008 there were 2,830 aged care homes delivering
residential care under these arrangements, with an occupancy rate of 93.86 per
cent over 2007-08. This compares to 94.5 per cent in 2006-07 and 95.2 per cent
in 2005-06.[20]
8.20
The ACAA argued that this declining occupancy rate has led to a context
in which there are 12 000 vacant places across the aged care system.[21]
8.21
Catholic Health Australia also noted that the planning and allocation
process fails to adequately reflect likely demand for places, particularly
residential care places and stated of the Aged Care Planning Advisory
Committees (ACPAC):
The ACPAC have only ABS Census data for the population 70
plus and between Census rounds the ABS and DoHA estimates by region and LGA.
The data doesn't always reflect actual population shifts, particularly in
geographic areas of high growth in older demographics. The methodology adopted
for determining ratios must be made transparent and should include assumptions
about socio economic status, access to services, ethnicity and expected
utilisation rates of services.[22]
8.22
Anglicare Australia also recognised that if planning ratios were set
with greater consideration of more localised social and demographic
information, clients in turn would have more information to make informed
decisions:
This would need to be accompanied by providing better
information to interested parties (existing and potential providers of both
residential and community care services; people who may be eligible for
assistance) on which to base their decisions on investments and care options.
It would also provide a platform to put more control and decision making power
in the hands of consumers rather than those of government and providers.[23]
8.23
Baptistcare amongst other providers highlighted the realities of family
relationships which impact on planning ratios. Of the current system,
Baptistcare stated:
It considers the numbers of aged people in a region and based
on those figures attempts to identify future need. It ignores changes that have
occurred in family relationships over recent decades and does not recognize
that people entering residential aged care are likely going to prefer residing
at a facility close to where their children live, rather than close to where
they previously lived.[24]
8.24
Mr Harold Milham of Alzheimer's Australia noted that the reform
proposals of the National Health and Hospitals Reform Commission to relate the
planning ratio with people rather than places was a means of breaking the
relationship between accommodation and care[25]
and providing greater choice for clients:
The approach to reform proposed by the National Health and
Hospitals Reform Commission has many elements that are in our submission to
your committee. We support the reform developed by the commission for
increasing choice in aged care by relating the planning ratio to people rather
than places, thus breaking the link between accommodation and care, and
providing choice for consumers for a mix of accommodation and care options;
basing the ratio on 85-plus, rather than 70-plus, to better reflect the
population group cared for; developing a national aged care program to provide
for the more effective integration of aged care services; and, finally, the
adoption of consumer directed models of care.[26]
8.25
The ACSA argued that the appropriate planning should take into account
three points:
-
The needs of older people for care
and housing extend beyond those provided under the Australian Government's aged
care program.
-
These needs need to be met in a
specific local area rather than 'in general', or 'statewide'.
-
The use of care services tends to
increase markedly with age.[27]
8.26
The Municipal Association of Victoria highlighted the need for consideration
of client characteristics and evidence of demand based on national datasets in
the establishing of planning ratios. Ms Kaye Owen explained:
In terms of a national aged-care planning framework, there
needs to be a coordinated development and use of supply, demand and utilisation
datasets. That fundamental need for data has been there for quite some time,
and it is an absolute necessity. There is opportunity to build on the local
area data and to incorporate a range of related program areas with agreed
processes with the three tiers of government and the involvement of providers
and consumers.[28]
8.27
Discussion on occupancy rates and differences between and within regions
exemplified what some providers viewed as an uneven distribution of places.
This reality has, according to Management Consultants and Technology Services
led to a situation in which there are 'serious shortfalls in places, and in
other areas of oversupply' in Victoria.[29]
The body concluded:
It would be of assistance to providers and assist them with
proper planning for places in appropriate allocations if they know where these
locations are. It would be helpful for all data at local LGA level to be
disclosed.
The current planning ratio should be an indicative model
only. For providers who wish to expand services to meet the true needs of their
community, there should be flexible model.[30]
8.28
The need for flexibility to meet local demand was also highlighted by
ECH Inc, Resthaven Inc and Eldercare Inc who stated that the current planning ratio
of 113 places per 1000 persons over 70 years of age should be retained but
that flexibility should also be introduced to the Aged Care Approvals Round to
enable variations in the residential and community care allocation ratio across
regions thereby enabling address of varying demand.[31]
8.29
On the other hand, Baptistcare argued for a market approach to planning
ratios:
The Governments targeted ratio of low-care, high-care and
community care places is excessively regulatory. There should be a market
approach, which will come to equilibrium between the three types of places
through the laws of supply and demand.[32]
8.30
Other concerns raised during the course of the inquiry centred on the
lack of information surrounding the establishment of current planning ratios.
According to the Western Australian Government, the calculation of the planning
ratios have never been explained:
The planning ratios are based on historically based planning
ratios that have evolved over time without a clear basis for their calculation
provided to the sector.
There has always been doubt associated with the calculation
of the planning ratios set in 1986 for low and high residential care for the
target population.
A transparent explanation has never been provided by the
Australian Government leading to concerns that the planning ratios have led to
an inherent systemic shortfall in allocated places in general over time.[33]
8.31
The planning ratios have not been comprehensively reviewed since they
were first introduced in 1985. The department itself noted that whilst changes
had been made to the ratios since their establishment, there have been
'significant demographic changes and changing patterns of use in aged care
services'.[34]
In terms of the changes, in 2004, in response to the Hogan Review, the Commonwealth
increased the operational provision ratio from 100 to 108 places for every 1000
people aged at least seventy, to be achieved in 2007. Further review in 2007
resulted in this ratio increasing to 113 places (88 residential and 25
community care) for every 1000 people aged 70 years or older by December 2011.
The balance of places within the provision ratio was also adjusted to increase
the number of community care places from 20 to 25 places for every 1000 people
aged at least seventy; four of these are for high level community care in the
form of EACH or EACH-D packages. Adjustments were also made within the
residential care target ratio of 88 places per 1000 people aged 70 years
or over to increase the provision of high care from 40 to 44 places.[35]
8.32
According to the 2008 Report on the Operation of the Aged Care Act
1997, the department is currently planning to initiate a review of the aged
care provision ratio.[36]
8.33
At the same time, however, Mr Andrew Stuart, First Assistant Secretary
of the department highlighted that:
There are very considerable strengths in the current planning
arrangements. We tend to take those for granted in Australia, but I think they
are very important to mention. First of all, the planning formula keeps growth
in care in line with growth in the ageing population and, secondly, the
planning formula directs new aged-care places to the areas of greatest need.
Aged care is really one of the very few areas in public policy where growth in
expenditure actually goes up in line with growth in the population. It is also
one of the few areas of public policy where growth in rural provision actually
matches the proportion of the population that lives in those areas. If you are
thinking about policy in the area of planning and allocation, you would not
want to lose those strengths that we currently have.[37]
8.34
The department also commented on arguments that a planning arrangement
based on 80 years of age rather than 70 years of age should be introduced to
more closely reflect the average age of residents. In response to such
suggestions, the department noted that:
-
a very good forward predictor of future demand is the population
aged over seventy. Despite impressions to the contrary, older people are not
highly mobile and they want to access care where they have been living; and
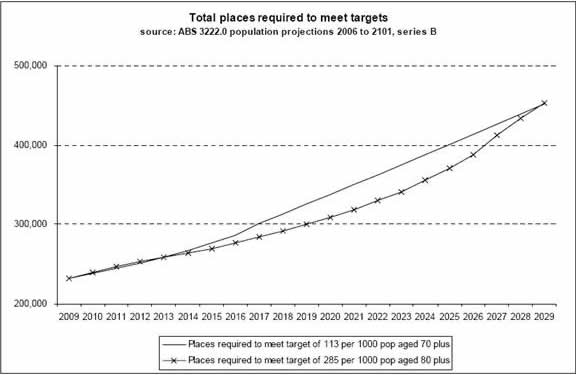
-
to move from a ratio based on seventy years of age to one based
on eighty years would soon (from 2013) produce a reduction in the release of
new places, and a concomitant saving in government expenditure, because growth
in this population will be less rapid than the total growth in those aged over
seventy. From the year 2021 there would then be a rapid surge in the number of
places required. This surge may challenge the industry's capacity to meet it
since it would produce a release of aged care places which is higher than any
release to date. The ratio based on those aged over seventy produces a steadier
growth path.[38]
8.35
The department provided the following graph to illustrate the latter
point.
Figure 8.1: Total places required to meet targets
8.36
The department also responded to comments concerning whether there is an
ongoing need for a distinction between low care and high care as there is
increasing utilisation of low care places by high care residents. The
department pointed to the distinction between accessing aged care services and
ageing in place.
8.37
In relation to access, the current aged care planning ratio for low and
high care are used for planning purposes and seek to ensure that places are
available for residents who need either high or low care on admission.
Currently, admissions are distributed evenly between high and low care (49.97
per cent entered as low care in 2007–08). According to the department, to
remove the ratio distinction between low and high care could result in reduced
access for low care residents.[39]
8.38
In relation to ageing in place, this policy is designed to enable clients
to remain in the same environment as their care needs increase where facilities
are able to offer the accommodation and care they require. Once a client has
entered care they are now generally able to remain in the same residential care
service as his or her care needs increase. As a result of ageing in place, the
number of care recipients who are actually receiving high level residential care
is significantly higher than 50 per cent. Indeed, as at 30 June 2008, some 69
per cent of residents in aged care homes were receiving high level care.[40]
8.39
The department went on to state that ageing in place is supported by the
current funding system with the ACFI a better and more objective measure of a
residents' care needs. With the introduction of the ACFI, the government has
allowed care needs to be reassessed at any time, so that significant increases
in frailty can be funded immediately. This further supports the policy
objective of ageing in place.
8.40
The department concluded:
In summary, policy over the last decade has consistently
emphasised relative growth in care at home, access to both
residential low care and high care, and the capacity for enduring care once a
resident is in the residential care setting.[41]
Conclusion
8.41
The committee recognises the new and emerging challenges facing the
industry in meeting growing demand and increasingly diverse client needs and
expectations. For this reason, the committee believes that it is timely for a transparent
and comprehensive review of the planning ratios. Such a review would provide an
opportunity to consider demographic and social information not currently
utilised and to deliberate on the impact of growing demands on the sector.
8.42
Such a review should consider the continuum of care as a long term
solution for the aged care sector and look beyond the distinctions between high
and low care. For this reason, the committee recommends that the suggested
taskforce review long-term options for the provision of aged care in Australia
including continuity of care.
Recommendation 30
8.43
The committee recommends that the suggested taskforce undertake a review
of the current planning ratio for community, high- and low-care places. Drawing
on all available demographic and social information, the review is an
opportunity to assess the planning ratio in light of growing and diverse demand
on aged care services.
Recommendation 31
8.44
The committee recommends that the suggested taskforce review continuity
of care as a potential long term solution for the aged care sector.
8.45
It should also be noted that witnesses drew a parallel between an effective
planning ratio and capital funding. According to the ACAA, the level of
investment in capital works ($1.45 billion in 2007–08) is not sustainable if
the Government continues to allocate places at the current rate and does not
assist with the cost of maintaining vacant places.[42]
Similarly, Aged and Community Services Association of NSW and ACT held that
planning ratios will not be effective until capital funding concerns are
addressed:
With expected increase in demand for higher levels of care in
the community the allocation of Extended Aged Care at Home (EACH) or EACH
Dementia (EACHD) would need to be increased. However changes in planning ratios
will not be effective if the underlying recurrent and capital funding
inadequacies are not addressed at the same time.[43]
8.46
Chapter 4 of this report considers the issue of capital funding in
greater depth.
Impact of current and future residential place allocations and funding on
community care places
8.47
With the growth in the number of older people living in their home for
longer periods of time, demand has risen for services in the community. The
Commonwealth provides these services through Home and Community Care (HACC)
programs, Community Aged Care Packages (CACP) and Extended Aged Care at Home
(EACH) Packages.
8.48
The department noted that in response to the increasing demand for
community care programs as an alternative to low or high level residential
care, the Commonwealth has been rapidly increasing the number of available
community care package places. CACP places increased 43.6 per cent over five
years from 2003–04, while EACH high care packages have increased nearly
five-fold since they were introduced in 2003–04.[44]
8.49
In evidence, some providers argued that the growth in community aged
care packages was leading to excess vacancies in residential aged care. Aged
and Community Services Association of NSW and ACT stated:
The consumer choice is towards community care, rather than
residential care and the current planning ratios may result in too many beds
for an aged population resulting in reduced occupancy rates and subsequent
viability issues.[45]
8.50
Emphasising growing client expectations to remain at home for as long as
feasible, Anglicare Australia argued for a change in the ratio between high and
low care:
Most people want, and have the means, to remain in their own
homes as long as possible, with an accompanying high demand for community based
care. This obviously reduces the demand for low level residential care. This
trend is likely to continue. This demands a recalibration of the planning ratio
to better reflect older people’s preferences and usage. The split between new
high and low level care residential places should be immediately shifted to
70:30, with future ratios being determined by actual and projected take up of
places.
This strongly suggests that the balance between residential
and community care needs re-examination, as does the provision of low and high
level care in the community (CACP and EACH) and the ease with which people are
able to transition from lower to higher levels of care in the community. The
current number of places available (for example, the Victorian ratio is 19.4
CACP places per 1000 population aged 70 years and over and 2.4 EACH places),
funding levels, as well as eligibility criteria for, CACP and EACH preclude an
easy transition, leaving many people no option but to enter residential care
before they are ready. There is a need for a continuum of care model to be
introduced, with greater flexibility to meet increasing levels of care need
and/or different care needs, and with planning ratios more accurately
reflecting likely demand for higher levels of care.
It is time to re-examine the level at which the number of
overall places is capped and whether ratios between residential and community
care need to be retained or could be abandoned, giving more flexibility in the
market.[46]
8.51
However, the Royal College of Nursing, Australia cautioned
the unintended consequences of emphasising community care:
Where feasible and safe, planning is
placing greater emphasis on providing community care services due to a
preference of many older people to remain at home for as long as possible.
However, the unintended consequences have seen a reduction in access to
residential care and a greater burden on families and carers who provide aged
care with little training; no supervision; meagre resources and at times having
to forgo paid employment to do so. Moreover, as people are remaining at home
longer, their overall condition can deteriorate to such an extent that when
they access aged care they require high care having not received the benefits
of good nutrition, informed care and essential treatment and skilled nursing
staff.[47]
8.52
The department responded to concerns about excess vacancies in
residential care resulting from a growth in community care. It noted that it
had not been able to produce analysis which supports or denies this view,
despite attempts.[48]
The department went on to state:
Intuitively, at some level, providing older people
with greater choice in care modality (in their own home or in an aged care
home) will lead to some reduction in interest in residential aged care.
However,
-
choice
in care setting is an explicit goal of policy; and
-
there
is evidence to show that people with high level needs who
are living alone and have no carer are more at risk of admission to
residential care (Australian Institute for Primary Care). Consequently there is
only a partial overlap between those who choose care at home and those who need
residential aged care.
The Department considers that the overriding dynamic in
explaining vacancy levels in aged care currently is not one of competition
between care types, but of rapid growth in care places leading to temporary
vacancies.[49]
8.53
The department went on to give an example of an area where a new
facility may be opened even though there are vacancies in existing facilities.
The department stated that the vacancy level 'will be a temporary effect
relating to growth' and concluded:
In situations like these, not all providers welcome the
expansion of aged care places but this expansion is essential to meet the
overriding public policy objective of meeting the growing demand of the ageing
population, which is expected to double in the next twenty years...
It is the Government’s intention to facilitate choice and to
continue to emphasise growth in care at home. Sufficient vacancies in both
community and residential care ensure people can get a place in the care of
their choice without undue delay; with providers competing amongst each other
to attract customers on the basis of quality of care and amenity.[50]
Conclusion
8.54
In light of the fact that the committee has recommended an overarching
review of the aged care sector and indeed supports a comprehensive review of
the planning ratios, it considers analysis of place allocations and funding as
integral to both such reviews.
Senator Helen Polley
Chair
Navigation: Previous Page | Contents | Next Page