Chapter 5
The current indexation formula
Introduction
5.1
This chapter considers the factors impacting on financial viability of
the aged care sector including increasing costs such as wages, construction
costs, changing consumer expectations and the adequacy of the current
indexation formula and specifically Commonwealth Own Purpose Outlays and the
Conditional Adjustment Payment (CAP) to address those costs.
Indexation formula
5.2
In aged care, the basic subsidy rates are adjusted annually in line with
movements in the Commonwealth Own Purpose Outlays (COPO). COPO indexation
arrangements came into effect in relation to residential aged care funding from
1 July 1996. COPO is weighted 75 per cent for wage costs and 25 per cent for
other costs and is calculated using the following algorithm:
COPO% = (annual CPI %
x 0.25) + (annual *SNA % x 0.75)
*SNA Safety Net Adjustment: SNA% = Safety Net Increase per
week/average weekly.[1]
5.3
As part of the Commonwealth's initial response to the Hogan Review, from
the 2004‑05 financial year, a Conditional Adjustment Payment (CAP) for
residential aged care was provided. CAP aims to provide 'medium term financial
assistance to residential care providers to assist them to become more
efficient, and more able to continue to provide high quality care to residents,
by improving corporate governance and financial management practices'.[2]
5.4
The amount of CAP payable in respect of resident is calculated as a
percentage of the basic subsidy amount payable in respect of a resident. In
2004–05, CAP was 1.75 per cent and then rose annually by 1.75 per cent
increments. CAP was initially introduced for four years and subsequently extended
for a further four years with no further annual increases so that the CAP is currently
set at 8.75 per cent. According to the Australian Government, this increase
will result in $2 billion in total CAP payments to the residential aged sector
over the next four years to 2011–12.[3]
5.5
In the 2008–09 Budget, it was announced that a review of the CAP arrangements would be undertaken to examine the CAP's effectiveness in encouraging efficiency
through improved management practices and the future need for, and level of,
this type of assistance. According to Australian Government, the findings of
the review will be submitted for consideration in the preparation for the
2009–10 Budget.
Adequacy of the current indexation formula
5.6
Concerns were raised by a number of witnesses regarding the current
indexation formula as its adequacy in compensating providers for the provision
of services impacts directly on their financial viability and their ability to
provide high quality services. The Aged Care Alliance submitted to the
committee, providers are constrained by static revenue flows based on subsidies
and periodic adjustments by mechanisms such as COPO. Providers have limited
influence over cost increases and no capacity to adjust the price of their
services.[4]
5.7
Mr Martin Laverty of Catholic Health Australia commented:
We would observe that there is not a mechanism by which the
market is able to inform the setting of prices, the provision of service and
the types of services that are provided, and nor is there an adequate mechanism
to determine what is an adequate Commonwealth subsidy to provide services for
those that do not have the capacity to meet the cost of the care themselves.[5]
5.8
The significance of indexation for providers was highlighted by Mr
Gerard Mansour of Aged and Community Care Victoria:
There is a whole range of cost drivers that impact on the
industry. So it is not surprising, given that we do not control pricing, that
the industry relies very heavily on indexation. It is like a slow death. If
indexation is gradually declining over time at any one point of change, then
the impact is marginal but the compounding impact of not meeting rising costs
is most significant. As I characterised it earlier, I hear very regularly about
how stretched and pushed the industry is and I have described it in a number of
places as being like the taut rubber band.[6]
5.9
It was argued by many providers that the current formula does not
adequately recognise the costs of the delivery of aged care services.[7]
Aged and Community Services Australia (ACSA) stated, for example, that the
indexation formula had resulted in a 'steadily widening gap between the costs
of providing a service and the subsidies provided by the Australian Government'.[8]
5.10
A major concern with the current indexation formula was that it does not
adequately take into account the cost drivers for aged care providers, in
particular wage increases. Some submitters commented that wages account for 70
to 80 per cent of their total costs. It was noted that annual wage increases
are generally between three and four per cent per annum. Aged and
Community Services SA & NT stated that the current indexation arrangement
was 'inadequate' because it 'does not actually reflect the health and aged care
labour market conditions'.[9]
The Australian Physiotherapy Association noted that indexation had not
maintained parity with salary increases in the health sector where competitive
salaries are necessary to ensure that sufficient numbers of appropriately
trained and qualified staff are employed in aged care to maintain quality of
service.[10]
5.11
Other costs such as groceries have increased about five per cent while
utilities have increased about 10 per cent per annum.[11]
Tasmanian providers, for example, indicated that they expected their
electricity costs to increase significantly (25 to 30 per cent) from July
2009 as they move into the retail contestible electricity market. Aged &
Community Services Tasmania noted that 'considering energy costs are in the top
five expenditure items for residential care facilities this has significant
implications for our sector in Tasmania'.[12]
5.12
Witnesses argued that present formula was impacting adversely on
provider viability and service provision. According to ACSA the indexation
system and system of user charging for the costs of accommodation in
particularly high care, has led to increasing numbers of residential aged care
services operating at a loss with all suffering declining returns.[13]
Capecare, for example, provided details of the impact of the current indexation
system's failure to recognise the actual costs of aged care:
The operating result has gone from a surplus of $7.03 per bed
per day in 2005/06 to a budgeted deficit of $11.37 in 2008/09. Wages and
related costs (leave provision, training, workers compensation, and
superannuation) make up 75% of all operating costs. Wages and related costs
have increased by 23% during these 4 years. Operating income had increased by
10% during the same period.[14]
5.13
Villa Maria, a non-for-profit operator of residential and
community-based care, commented:
Continued pressure for wage related increases are
outstripping fee increases, creating a growing area of concern about long-term
financial viability. Essentially, the indexation applied to subsidies is not
maintaining relativity to wages increases.[15]
5.14
The Brotherhood of St Laurence (BSL) also submitted that the inadequacy
of the current indexation is demonstrated by the BSL's current Enterprise
Bargaining Agreement which allowed for an annual salary increase of 4 per cent
for staff and the current annual increase of most supplies in excess of 4 per
cent. The CPI increase for the year to September 2008 was 5 per cent and the
annual COPO increase was around 2.3 per cent. This left a gap of around 1.7 per
cent which for the BSL meant a funding shortfall, in terms of indexation only,
of nearly $98,500 for the 2008‑09 financial year. The BSL stated that
these figures take into account the CAP.[16]
5.15
Submitters argued that the impact of the shortfall in subsidies has led
to service providers seeking savings in operation costs. Anglicare noted that
the rationing of services impacts particularly on older people with limited
means and limited alternative supports.[17]
5.16
Submitters also argued that the current indexation formula for community
based services has not kept pace with costs, particularly travel costs for
home-based services. For example, Bromilow Home Support Services stated that
there has been a reduction in services hours provided to clients and commented
that 'it is impossible for service providers to maintain consistency in the
service levels provided to clients from one year to the next when subsidy
levels continue to fall in real terms'.[18]
Care Connect commented that the annual packaged care subsidy increase, as
determined by the COPO index has fallen behind the annual rate of increase in
unit costs of providing care and operating services. As a result, the amount of
care that can be purchased per package has been severely eroded over the last
ten years.[19]
5.17
NCOSS similarly commented that the existing indexation method is
inappropriate for community care, as it does not reflect the real staffing and
other costs of running services. NCOSS also noted that the indexation for
Community Aged Care Packages and HACC are calculated in a slightly different
way for each program resulting in different levels of compensation for similar
cost increases.[20]
Aged Care Queensland also noted that services such as Day Therapy Centres have
lower levels of COPO indexation applied, with that result that Day Therapy
Centres received 2 per cent indexation and other community care programs
received 2.2 per cent.[21]
5.18
Evidence was also provided to the committee concerning the long-term
impact of the current indexation formula on the sector. According to the House
Group of Companies, the real value of COPO has eroded 23.5 per cent over the
past eight years, which means according to the group, 'a continued
deterioration of our sector's viability in the long run'.[22]
5.19
Mr Peter Wright of Anglicare Aged Care South Australia commented:
I would like to reiterate that we have experienced our costs
rising faster than CAP and COPO combined. In effect, we are going backwards,
because our costs are exceeding the reimbursement or the indexation method that
is employed. You probably have the paper by the Aged Care Industry Council,
which gave a very good summary of the shortcomings of the COPO and the CAP. It
is very poignant to point out, without going through the detail of that paper,
that COPO/CAP increases are actually less than the safety net adjustments and
also the average weekly overtime earnings adjustments. We are well behind some
key benchmarks.[23]
5.20
The Aged and Community Services Association of NSW and ACT held that
whilst the CAP was not introduced for community aged care, COPO does not
adequately recognise increases in wages with the result that purchasing
capacity of a Community Aged Care Package (CACP) has diminished considerably
since 1994:
Between 1995/96 and 2005/06 the value of the package had
increased by 27%, yet the overall increase in the ordinary time earnings of
full time working adults has been 64%, more than double the increase in CACP
subsidy.[24]
5.21
Alzheimer's Australia cites the Aged Care Industry Council submission to
the CAP Review to demonstrate that the indexation of CACPs, EACH and HACC has
been at a level below the increase in labour costs:
...from 1996–7 to 2003–04, the Commonwealth's "COPO"
indexation formula meant that the CACP subsidy increased by 21.6%. During that
same period, ordinarily time earnings for full time adults increased by 47.3%.
Indexation of community care subsidies needs to be based on
the labour component. The Conditional Adjustment Payment should be paid
immediately to community care services. Continuation of CPI indexation simply
means fewer services being provided as increase in wage costs eat into service
provision hours.[25]
5.22
According to NCOSS, the growth of the HACC program has been compromised
by inadequate indexation. Citing the Aged and Community Services Association of
NSW and ACT, NCOSS maintained that the indexation method does not reflect the
true costs:
...estimating that, between 1999–2000 and 2001–02, the HACC
Program in NSW had been underfunded by between $17.6m and $28.5m. Indexation
for the same period to HACC services in NSW was estimated at 6.36% according to
the COPO method; other indices suggest a figure closer to 14% for increases in
costs for this period.[26]
5.23
The Department of Health and Ageing (the department) responded to these
comments and noted that the Government has provided substantial increases in
funding for residential aged care. The expenditure in 2008–09 is estimated to
be $6.7 billion which represents an increase of some 10.8 per cent over
the expenditure of $6.0 billion in 2007–08. In 2008–09, Government funding for
each day a resident spends in residential care will be about 8 per cent more
than it was in 2007–08 for a resident of the same level of frailty. This growth
reflects the increases in funding accompanying the implementation of the new
Aged Care Funding Instrument (ACFI) and funding changes to accommodation
charges and supplements introduced on 20 March 2008.
5.24
The Government made changes to enable increases in accommodation
payments – both government subsidies and user contributions – particularly in
high care. Overall these changes will deliver increased revenue to the
residential care sector of more than $750 million over four years, including
more than $480 million in increased government subsidies. In 2008–09, the
changes will result in an increase from the Commonwealth of more than $267
million in residential care funding. Once fully phased in the changes will
deliver more than $350 million per year in increased revenue, mostly in respect
of high care residents, to support investment in high care facilities.
5.25
The growth in Government funding to the residential aged care sector
reflects indexation and the Conditional Adjustment Payment, population growth,
increases in frailty and changes in policy. Net funding growth has been 8 per
cent per resident. The contribution of various factors to this total growth for
2008–09 is as follows:
-
indexation contributed 28 per cent;
-
CAP contributed 18 per cent;
-
frailty growth contributed 17 per cent; and
-
new policy contributed 37 per cent.[27]
5.26
The department also noted that developed cost and revenue indices for
both high- and low-care providers to look at the comparison of cost to revenue
for both low- and high-care homes. Mr Stuart commented that the revenue has
been increasing faster than cost since 1998–99. The department provided the
following comparison of the growth of revenue indices with the growth in cost
indices. The data is presented on an index basis with revenue and cost for
1998–00 set to 100.
Graph 5.1: Unit cost and revenue growth (constant frailty) –
low care
Graph 5.2: Unit cost and revenue growth (constant frailty) –
high care
Source: Department of Health and Ageing, Supplementary
Submission 114a, p.26-27.
5.27
Mr Andrew Stuart from the Department of Health and Ageing commented on
the difference in the department analysis and that of the sector:
I think I should explain that the main difference between
what the department has been doing in this area and what the industry has been
doing is that the industry has been comparing revenue to prices, in particular
labour prices, on a per-unit basis, and the department has taken account of
productivity improvement in looking at the relationship between revenue and
cost.[28]
5.28
Dr David Cullen, from the department also made these comments:
What we do know and what we have
given in evidence here is that, for the last 10 years—and we have only gone
back 10 years in our data—revenue has grown faster than cost. So, if that is
the case, if revenue has grown faster than cost and if, as we have given you
evidence, the average payment per resident this year is eight per cent greater
than the average payment per resident of the same level of frailty last year,
that would seem to indicate that the problem is not on the revenue side.[29]
And further:
The fundamental difference between the department’s analysis
and the industry’s analysis is that the industry looks at what would be called
the unit costs of inputs and says, ‘How much does a unit of import go up?’ We
look at the unit cost of outputs. We say, ‘How much does it cost to produce a
day of care?’ When you are producing a day of care, or in any industry, each
year you make productivity improvements. It becomes cheaper to produce care one
year on the next because of productivity improvements. We take that into
account; they do not.[30]
Use of COPO and CAP
5.29
According to witnesses the reason for the inadequacy of indexation in
the aged care sector is the use of COPO and its failure to recognise actual
costs in the industry. These problems have been longstanding and the
compounding impact over the last decade has resulted in increasing negative
impacts on the sector. Mr Greg Mundy of Aged and Community Services Australia
stated:
In terms of...the indexation formula, that is one of two main
contributors to that scenario. It has been not a sudden development but a
steady development over a long period of time that the value of the
Commonwealth's subsidies for care has not kept pace with the cost of providing
that care. The main reason for that is that the way the government measures
wage cost increases is based on what we used to call the safety net adjustment,
now the Fair Pay Commission adjustment. Health staff are in relatively short
supply, especially but not only nurses, and they have done better than that
adjustment over a long period of time. So there has been a steadily widening
gap between what it costs us to provide services and what the subsidies will
cover.[31]
5.30
Many submitters voiced the same concern as Mr Mundy about the
recognition of wage increases. Submitters noted that over the past 10 years the
subsidy increase have averaged approximately two per cent per annum which is
far below annual increase in wages and other cost inputs.[32]
In addition, it was noted that the Commonwealth uses the Safety Net Adjustment
rather than actual aged care sector wage increases which have occurred as a
result of enterprise bargaining, to determine COPO.[33]
The result of this, according to Care Connect, in a method of indexation 'insufficient
to maintain pace with real increases in the costs of running businesses and
providing care'.[34]
5.31
The concerns about the recognition of wage movements are longstanding.
In its 2008 report, the Productivity Commission made the following comments on
COPO:
A longstanding concern of the aged care industry has been
that the indexation of basic subsidy rates is not based on movements in
industry-specific costs. Rather, subsidies are indexed using the Commonwealth
Own Purpose Outlays (COPO) index, which is weighted 75 per cent for wage costs
and 25 per cent for non-wage costs. The COPO is premised on the view that
virtually all wage increases are productivity based. Hence, it only makes
provision for safety net increases in wages and for economy-wide movements in
non-wage costs. Thus, if productivity gains within the aged care sector do not
keep pace with other sectors, the subsidy, as indexed, will be increasingly
inadequate.[35]
Comparison of aged care indexation
with other indices
5.32
Submitters provided the committee with comparisons of the current
indexation compared with other indices. Aged and Community Care Australia
provided the following comparison of combined COPO/CAP subsidy to SNA – Minimum
Wage and AWOTE.
Table 5.1: Comparison of COPO, CAP, SNA and AWOTE
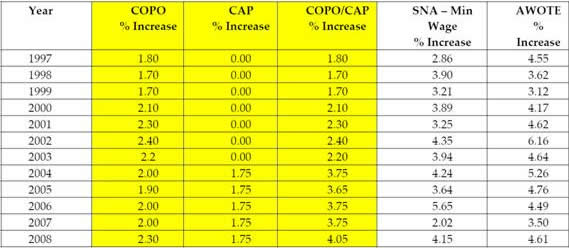
Source: Aged and Community
Care Australia, Submission 92, p. 16.
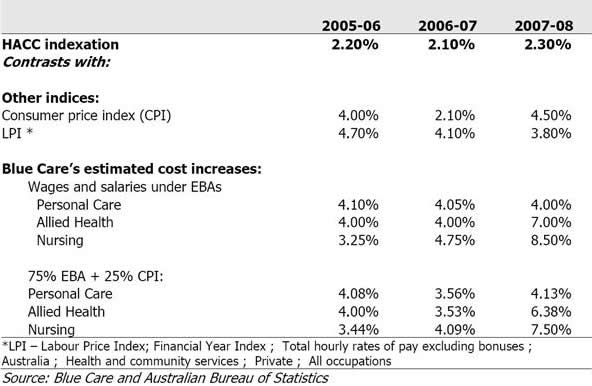
5.33
Blue Care provided the following analysis of HACC indexation.[36]
Table 5.2: Comparison of HACC indexation with other cost
indices and Blue Care's input cost increases
5.34
Witnesses also noted that the Department of Veterans' Affairs is
understood to have abandoned the COPO index for its Veterans' Home Care program.[37]
The BSL commented:
It is clear that the current COPO indexation is inappropriate
for the Aged Care industry. The Veterans' Home Care program does not use the
COPO index and private health insurance premiums have had much higher increases
authorised by successive Ministers for Health, which have actually fuelled wage
growth.[38]
The Conditional Adjustment Payment
5.35
The committee was provided with evidence on the importance of CAP to the
aged care sector. It was noted by Catholic Health Australia that CAP was a
significant factor in maintaining subsidy levels close to the CPI:
Most notably, increases in both High care subsidy rates
(average 3.5% per annum) and Low care rates (average of 3.7% per annum) only
kept pace with CPI growth and, indeed, slightly exceeded it when topped up by
the CAP payment set at 1.75%.[39]
5.36
Witnesses noted that the CAP was intended as a temporary measure but for
many providers CAP was required to maintain their viability. The Aged Care
Alliance noted that 'the effects of external costs, the inadequacy of COPO and
workforce issues have created high dependence on its [CAP's] continuation'.[40]
UnitingCare Australia, which provides residential aged care to approximately
6,900 elderly people representing approximately four per cent of funded
residential aged care beds, noted that without the temporary CAP:
...losses may have already resulted in UnitingCare withdrawing
from the provision of residential aged care services. In the absence of
substantive positive funding reform this will occur.[41]
5.37
Indeed, UnitingCare Australia maintained that had the CAP not existed, its agencies would have lost $36.5 million from the time of the introduction of
the CAP to the end of the 2008–09 financial year. Consequences of removing the CAP for UnitingCare Australia agencies may include:
-
withdrawal from the provision of
residential aged care (closure of existing facilities);
-
deferral/abandonment of new
investment (already happening);
-
refurbishment of run-down
facilities rather than replacement (already happening);
-
relinquishment of provisional
allocations of residential care places and not proceeding with new capital
investment (already happening).[42]
5.38
Concerns were raised in a number of submissions that the CAP is now effectively frozen for the next four years with no annual 1.75 per cent increase.
According to Management Consultant and Technology Services and Baptcare,
without the annual increase adjustment, the aged care industry cannot further
stretch COPO funding increases, which are already less than costs, and have
been eroded 23.5 per cent over the past eight years.[43]
They maintain that this freeze will result in a drop of funding of $750 per
resident per annum. The Aged Care Association Australia – SA commented that 'at
best, CAP has prevented further erosion in the real value of subsidies, but has
gone no way to offsetting the significant erosion which accumulated during the
years before the introduction of CAP'.[44]
5.39
Aged Care Association Australia WA and Aged and Community Services WA
also noted that the reporting requirements for the CAP were considerable whilst
the industry had not been provided with any certainty that the payments will
continue in coming years.[45]
5.40
Alzheimer's Australia maintained that the 'biggest anomaly' of the
indexation system was in relation to community aged care:
Community care has a very high proportion of its costs as
labour costs, but the indexation of CACPS, EACH and HACC ahs been at a level
well become the increase in labour costs. The additional funding that flowed to
residential care as a result of the Conditional Adjustment payment (CAP) did not flow to community care, despite its higher labour costs.[46]
5.41
COTA Over 50s also noted that the CAP has not been applied to the
community care program despite the cost pressures which it maintains are
similar to that in residential care.[47]
The Aged and Community Services Association of NSW and ACT held a similar view,
stating that the CAP should be extended to community care programs from 2009.[48]
Calls for an improved indexation
formula
5.42
Witnesses argued that there was a need for a new indexation formula
which adequately addresses the sector's needs. The BSL for example, commented
that:
A new long term indexation formula needs to be introduced
which accurately captures all the cost drivers such as wage increase, consumer
items, building costs and energy and water prices.[49]
5.43
Mr Stephen Teulan, UnitingCare Australia, commented:
Unless indexation of subsidies improves in terms of the way
that it is calculated or in the meantime if the conditional adjustment payment
does not continue there is going to be a huge hole in the budgets of every
residential aged care provider in Australia.[50]
5.44
The committee received a number of suggestions as to how the indexation
formula could be improved. CHA recommended the introduction of a new benchmark
weighted at 75 per cent for wage growth and 25 per cent for non-wage growth,
using the Labour Price Index (Health and Community Services) for the wage
element and the CPI for general prices.[51]
5.45
Blue Care submitted that future indexation formulae should:
5.46
An industry specific indices, or an 'Aged Care index', was also
supported by other submitters.[53]
According to Baptcare, a long term 'aged care index' which properly recognises
all cost drivers, wage growth, consumer items, building costs and increased
energy and water prices is required.[54]
Similarly, the Aged and Community Services Association of NSW and ACT held that
a specific residential aged and community care index should be developed and
applied annually in order that movements in the average cost of care are
covered each year. According to the association:
This could be administered by an independent body, analogous
to the Fair Pay Commission, to ensure transparency and to avoid conflicts of
interest.[55]
5.47
Submitters also supported the extension of CAP to community care
services.[56]
Conclusion
5.48
Witnesses raised grave concerns about the adequacy of the indexation
formula used by the Commonwealth for both residential and community aged care, particularly
in relation to addressing wage increases. The committee considers, on the
balance of the evidence before it, that the current indexation formula may no
longer be appropriate for the aged care sector. The committee therefore
considers that the formula needs to be reviewed and modified if required. The
suggested review of the benchmark of care costs, as detailed in Chapter 3,
should inform this review.
Recommendation 14
5.49
The committee recommends that the taskforce undertake a review of the
indexation formula used for the aged care sector in order to identify its
adequacy in relation to costs faced by the sector and to identify modifications
to the formula if required.
5.50
The committee further recommends that consideration be given to an
independent mechanism to continually assess the indexation formula.
5.51
The committee also acknowledges that a review of CAP is presently being
undertaken. The committee strongly urges the Commonwealth to consider the
continuation of CAP whilst the recommended all-encompassing review is being
undertaken.
Navigation: Previous Page | Contents | Next Page