|
Navigation: Previous Page | Contents | Next Page
Chapter 2
The Barwon trial site
2.1 This chapter presents the committee's evidence on the achievements and the challenges facing the National Disability Insurance Scheme (NDIS) in the Barwon trial site in Victoria.
The public hearings
2.2 The committee held public hearings in Geelong on 14 and 15 April 2014. On 14 April, the committee took evidence from 20 participants, 1 carer and 15 service providers. On 15 April, the committee heard from Victorian Department of Human Services officials and Victorian-based National Disability Insurance Agency (NDIA) officials. A list of those who gave evidence in Geelong is at Appendix 1. The transcript of evidence from these hearings is available on the committee's website. The committee thanks all who gave evidence to the committee in Geelong.
2.3 On 14 April, the committee held two sessions 'in-camera': the first took evidence from participants and carers in the Barwon trial and the second from service providers.
2.4 The committee's public hearings in Geelong raised a number of issues specific to the progress of the Barwon trial site, as well as various broader themes common to all the trial sites. These themes are developed in chapter 6 of this report.
Progress of the Barwon trial site
2.5 The Barwon trial site commenced on 1 July 2013 covering the local government areas of the City of Greater Geelong, the Colac-Otway Shire, the Borough of Queenscliffe and the Surf Coast Shire.[1]
2.6 Table 2.1 presents the statistics of the Barwon trial site until 31 March 2014. It shows that the bilateral agreement between the Commonwealth and Victorian Governments planned for a total of 4,076 participants over 2013–14 in the Barwon trial site. As of April 2014, there had been 3,108 access requests, 2,495 participants had been accepted into the Scheme, and 2,113 participants had plans. On all three performance measures, the Barwon trial site had the highest numbers of any trial site.
Table 2.1: Key statistics of the Barwon trial site (after 9 months)
|
Barwon |
South Australia
|
Tasmania
|
Hunter
|
|
Number of participants in bilateral agreement
|
4,076
|
1565
|
792
|
3000
|
|
Number of participants with plans, 31 March
|
2,113
|
979
|
585
|
1,724
|
|
Access requests
|
3,108
|
1,449
|
744
|
2,720
|
|
Accepted as eligible
|
2,495
|
1,152
|
685
|
2,042
|
|
Ineligible (i)
|
205
|
116
|
19
|
461
|
|
Other (ii)
|
613
|
297
|
59
|
217
|
|
Average days from access request to plan approval
|
49
|
51
|
56
|
54
|
|
Average time from application to commencement of services
|
101
|
76
|
90
|
79
|
|
Review of decisions
|
26
|
12
|
-
|
14
|
|
Participants accessing mainstream services (% of total)
|
92
|
88
|
76
|
68
|
Source: National Disability Insurance Agency, Quarterly Report to COAG Disability Reform Council, 31 March 2014.
(i) This figure relates to the intake for the 12 months from 1 July 2013.
(ii) This is a combination of 'in progress', closed', 'revoked' and 'withdrawn'.
Transition to the NDIS in the Barwon trial site
2.7 Unlike the Hunter trial site, which is phasing by provider and local government area, and the Tasmanian and South Australian trials, which are phasing by age cohort, the Barwon trial site is phasing by program. Table 2.2 shows the phasing schedule for the Barwon trial site. It plots the process through which the Victorian Department of Human Services (DHS) intends to transition its clients to the NDIS. Its first priority was to transition those people on the Disability Support Register (DSR) and Early Childhood Intervention Services waiting lists. DHS explains on its website that:
The DSR is a database of all the people with a confirmed need for funding (an Individual Support Package) to purchase supports that meet their disability needs or for supported accommodation. The Register is used to allocate these supports in a fair and efficient manner when funding or vacancies become available. The number of people recorded on the DSR as at 31 December 2013 is shown in the following table.[2]
|
DSR Category
|
All Requests
|
|
All requests
|
1,374
|
|
Supported Accommodation
|
2,865
|
|
Total
|
4,239
|
Source: Victorian Department of Human Services
2.8 Early Childhood Intervention Services are funded by the Victorian Government to support children with disability or developmental delay from birth to school entry and their families. The services, ranging from special education to therapy and counselling are provided by Specialist Children's services teams and Early Childhood Intervention agencies.[3] Under the NDIS, these services will be transitioned to not-for-profit and private providers.
Table 2.2: Transition arrangements in the Barwon trial site
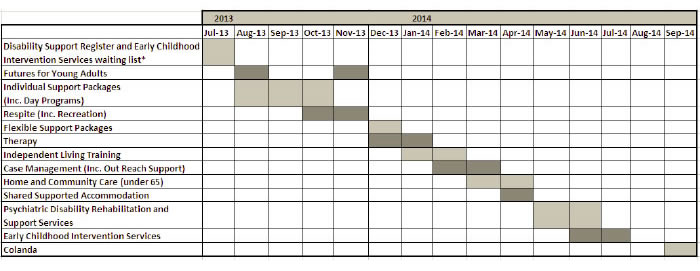
*Disability Support Register and Early Childhood Intervention Services waiting list from 15 April 2013.
Note: Funding for disability services Training and Development and Industry Development and Innovation will be transferred to the Scheme in September 2013.
Source: Victorian Government, Department of Human Services
Achievements of the Barwon site to date
2.9 The committee heard from the Barwon trial site manager, Ms Stephanie Gunn, that there have already been some important achievements in the site. These are:
- there are no Disability Services Register or Early Childhood Intervention Services waiting lists;
- core supports are being delivered;
- there is evidence that service providers are adapting and responding to the complex needs of participants; and
- there is NDIA survey data showing a very high level of participant satisfaction with the planning process.
No waiting lists
2.10 The transition of people with disability from the DSR and Early Childhood waiting lists into the NDIS was an early objective of the trial site (see Table 2.2). One of the early achievements of the Barwon trial was to achieve this transition. As Ms Gunn told the committee:
It is important to acknowledge the fantastic systemic changes that are being achieved and note that there is no longer a waiting list. People on the DSR in Victoria have waited seven years, and they only got on the DSR because of their high and intense acknowledged need. There are no waiting lists for children needing early intervention. This is really important. Children under six are no longer waiting for early intervention supports. That means that we are catching them early, we are providing the therapy and the support to their families and, with a bit of luck, we will not see them going forward into the system. If we do, their needs will be greatly reduced. We are giving them the best opportunity from the start.[4]
2.11 Ms Gunn told the committee that the vast majority of the trial site's intake will be completed by October 2014.[5]
Delivering core supports
2.12 A fundamental challenge for every trial site is to ensure that equipment is readily available for participants. In Victoria, the supply of equipment is the responsibility of the State-Wide Equipment Program (SWEP). SWEP is responsible for meeting participants' approved assistive technology needs through purchasing, customising and supplying the loan of items to participants.[6]
2.13 The committee heard that in the Barwon trial, core supports have been provided for NDIS participants and choice and options for people with disability are starting to emerge. Ms Gunn told the committee:
Core supports have been addressed-things like personal support, continence aids and equipment. Many people have waited many years or have survived with very low levels of those supports in their lives. Sustainability of the support provided by families is being strengthened by a range of different strategies.[7]
2.14 The NDIA acknowledged the role of SWEP in providing core supports for participants. While noting this role, the Barwon trial site manager told the committee that SWEP will in time be replaced and that the NDIA needs to retain purchasing power for its equipment needs:
The work and support that SWEP have given us has been phenomenal, and we are very grateful for that. That has meant that the vast majority of our equipment decisions in people's plans have been filled really rapidly and that has addressed many gaps and the waiting lists and all of those things have been improved. There are delivery delays sometimes and the focus from the national office is developing a national aids and equipment strategy. That project is now well under way and it is working collaboratively with all of the jurisdictions to take the best of breed around their aids and equipment programs. I am not sure of the time line of when that is going to be kicked out, but certainly the recognition that the purchasing power of the agency for aids and equipment needs to be exploited for the benefit of the scheme is very well accepted by the agency.[8]
Innovative service delivery
2.15 Ms Gunn also told the committee that service providers in the Barwon trial site have been adapting and responding to the complex needs of participants in the Scheme. She explained to the committee that:
There are some fantastic things happening. There is expansion. There are some amazingly innovative, committed supports being provided that we have never seen in this area previously. There is in particular a group of providers who are standing up and offering to provide the most extraordinary services for people with complex behaviours and behaviours of concern. When you read the history of the individual and the journeys that those individuals are now on with these supports, they started very slowly under the previous government's support through ISPs—I do acknowledge that—but are increasingly supported by some providers under our scheme. They are fabulous stories.[9]
2.16 The committee has not yet had the opportunity to observe first-hand the types of services to which the Barwon trial site manager refers. However, it has received evidence from several service providers in the Barwon region about the type of services that they provide and the challenges that they are facing in making the transition to a 'fee-for-service' model (see below). The committee also heard very positive stories from NDIS participants that corroborates Ms Gunn's testament.
Positive feedback from participants
2.17 Ms Gunn noted that the NDIA conducts a satisfaction survey in which '95 per cent of participants rated their experience with the planner, the engagement, the process and the outcomes either good or very good'.[10] The results of this survey are presented in Table 2.3 below. The committee recommends that the NDIA could improve the presentation of this information (see recommendation 9).
Table 2.3—Participant feedback
|
YTD
|
Total responses
|
Very good
|
Good
|
Neutral
|
Poor
|
Very poor
|
|
Overall, how would you rate you experience with the planning process today?
|
784
|
571
(73%)
|
169
(22%)
|
33
(4%)
|
10
(1%)
|
1
(0.1%)
|
|
NSW
|
179
|
148
|
27
|
4
|
0
|
0
|
|
South Australia
|
272
|
157
|
83
|
21
|
10
|
1
|
|
Tasmania
|
58
|
52
|
6
|
0
|
0
|
0
|
|
Victoria
|
275
|
214
|
53
|
8
|
0
|
0
|
Source: National Disability Insurance Agency, correspondence received 8 July 2014.
2.18 The committee did receive some very positive stories from participants and their carers about the planning process in the Barwon trial site. Mr Kevin Stone, an advocate for the Victorian Advocacy League for Individuals with Disability (VALID), told the committee:
...I am a parent of a man who is a participant in the NDIS. Damian is 43 years old. He lives in a group home in Grovedale. My experience as a parent going through the process was a very seamless one, largely due to the fact that we had a wonderful planner who had had a lot of experience previously in person-centred planning. She sat down with us as a family and with my son and went through the goals, aspirations and talked about his needs and collaboratively developed a plan that we all felt really happy with. It then proceeded through and we were delighted with the outcomes.[11]
2.19 Ms Simone Stevens, an NDIS participant, was glowing in her assessment of the Scheme. She gave the following account to the committee:
I am on a very good package at the moment with the NDIA. I was getting 21.1 hours before, and now I am getting 42 hours. I am doing a lot more. I can be more flexible. I work up in Melbourne with Kevin [Stone]. It has given me great flexibility and good insight with carers and my coordinator, and now we can just do that, because I can do more. Without the NDIA, I would not be able to do that. I am just amazed at how great things are at the moment.[12]
2.20 She added:
It is incredible. I cannot believe it. I cannot believe how incredibly happy I am at the moment, so it is great...
I am getting a new manual wheelchair too, thanks to the NDIA, so it is really good.
The goals were what I wanted to achieve in my life. I am actually quite blessed. I got in contact with my friend who I had not seen in 19 years, and so now I spend—I think it is—every month up in Camperdown. I am able to go up and visit her, whereas before I was not able to because the funding would not allow it. But now I can go up and see her. That has really helped. I think that is the most important part of the goals. The other part of the goals was the work side of it. I am very work related. I love to do whatever I can to work whenever I can. If I am not working, if I am sitting around at home, I get very annoyed very quickly, so I have got to be up and around and moving, going up to Melbourne, working in Geelong, doing whatever. But I have got to be moving all the time. Without the NDIA and without the goals, I think I would be very stuck.[13]
2.21 Ms Bianca Brant gave evidence in Geelong on her experience in securing a package for her six year old son, Tom. Tom was one of the first children to be signed off for a plan and a package in the Barwon trial site. Ms Brant stated:
We had a really good planner... I said to her straight away that I would like to tell the story once and could she take notes and then put it into the table for me because I was going to find it overwhelming and get emotional—or that is what I was worried about. She was good. I told her what my goals were for Tom and for me. She had an ability to sort of step into my shoes.[14]
2.22 Ms Brant also noted that self-managing her son's plan was empowering:
I had case management as one of my things for Tom's plan, because I wanted to be able to step back a bit and just be the mum and less of an administrator and nurse and everything else. But it actually did not work out. I found it very frustrating that my case manager was, I felt, pushing emails around and not really solving issues. I ended up sacking her, which was really empowering—you can do that. So you are not necessarily stuck with someone. I thought the person was very experienced because they had done it before and they were in an organisation that had been around for a long time. They were happy to take the money but I said, 'I want to know what you are actually doing.' There did not seem to be much evidence of that, so that ceased and that was good.[15]
Challenges in the Barwon trial site
2.23 The committee heard a range of criticisms from participants, their carers and service providers about the rollout of the scheme in the Barwon trial site. Ms Gunn herself acknowledged that there have been complaints which relate 'largely to eligibility, issues around the health interface, our timeliness in resolving issues that are raised and the overall planning outcomes that they have had'.[16]
2.24 The committee notes that the challenges of the Barwon trial site relate mainly to the NDIA's processes, its culture and its communication with stakeholders. The rest of this chapter presents the committee's evidence on the following issues:
- the planning process and the lack of flexibility in plans;
- the NDIA's information technology system;
- participants' problems transitioning from Individualised Support Packages (ISPs) to the NDIS;
- the culture of the NDIA;
- the composition of NDIA staff;
- problems with transport for both participants and service providers;
- service providers and the costs of the fee for service model;
- cross-subsidising and fee gouging;
- incorrect plans;
- mental health and the financial viability of service providers;
- NDIA's lack of responsiveness to service providers; and
- housing issues.
The planning process and the lack of flexibility in plans
2.25 A principal concern of several participants and their carers in the Barwon trial site was the lack of flexibility in plans in the event that a participant wished to change their day-to-day arrangements.[17] While the problem is systemic and relevant to participants in all trial sites, the issue was raised repeatedly at the public hearing in Geelong on 14 April.
2.26 The committee heard that participants had been unable to make even minor amendments to their daily activities without first having to change their plan. Mr Stone told the committee that the planning process is 'far too rigid', 'very confusing' and also referred to issues with the IT system.[18] Ms Marge Knight, who manages her son's plan, told the committee that the inflexibility of plans is contrary to the Scheme's broad principles of choice and control:
While the previous model enabled myself to redistribute moneys allocated to each flexible support as required, the new, more rigid model provides no such flexibility. This rigid model inhibits Andrew's support needs, should unforeseen circumstances arise; impedes Andrew's capacity to participate in impromptu social activities or desired appointments, as is the nature of any person's changeable lifestyle; denies full control over Andrew's funds to which he has already been approved; and disregards the very principle of choice, control and presumption of capacity and design....
[I]t is about me being able as an administrator or an advocate for Andrew to utilise those funds for him with flexibility and not being structured into a line of funding. As I think has been touched on before, certain amounts get dropped into each line per month and then you are allocated that money to be able to spend it. That does not allow us any control or flexibility to meet his needs.[19]
2.27 The committee asked the NDIA to comment on this issue. Ms Gunn told the committee that:
The line-by-line approach was very much designed, particularly in the supports and community access arrangements, to incentivise providers to offer supports in non-standard hours, because, as many participants will have told you over many years, there is limited support in being able to get flexible provision. Having said that, the actuary's advice was to
de-aggregate the price. So, in Victoria there was one price across all hours, and we offer very different prices for different hours and different times.[20]
2.28 Ms Gunn also attributed part of the problem for the inflexibility of plans in the Barwon trial site to the mindset of planners and the Agency itself. However, she indicated that this was changing to better reflect the individual's needs:
When we started we had new staff from many different backgrounds with different cultures, values, skills and experiences; we had a new IT system; we had new legislation that had no case law to guide us; we had limited practical considerations and expansion of the issues that we wanted to explore within the legislation. I think that our actions have swung to one side-to the letter of the legislation, to ensure our compliance, rather than to the intent. With our learning commitments, our sharing across our sites, the gathering of data and the development of evidence, we are now seeing our ability to move back the other way-more into that centre-to be more flexible, innovative and responsive to individual need. We are confident of that. We will need the support of the community and the government in acknowledging that there will be great inconsistency in the plans that we produce because that is what having an individualised, family centred and person centred planning process means.[21]
2.29 The committee notes that NDIS participants are not necessarily seeking more financial support than they had under their previous arrangements. Indeed, Ms Knight explicitly told the committee that the quantum of money was not her concern in terms of providing supports for her son. Rather, the key issue for her was to access and use of her son's existing funding:
Three weeks ago I rang the planner and said: 'We really do need to talk. I need to be able to find out how I can access these funds to get my son to be able to do the main thing in his life to get him back on balance.' I said to them: 'I don't want any more money; I just want to access what you have given me.' Then I had a phone call, saying: 'I have some great news. You have got some more money.' I said, 'I don't want more money. Just let me access what I've got.' They have given me this massive amount of money. I said, 'That's great, but how do I get him there?' And they said, 'Don't you have support staff?' I said: 'Yes, but it is their cars. How do I find these people?' That is great and I appreciate that and that is a problem for me is to sort through. But they have dumped more money into Andrew's allowance rather than me being able to use the money I already had.[22]
2.30 Ms Brant told the committee of her difficulties in rearranging respite care days for Tom after an operation on his legs. Ms Brant had regular carers she used for Tom and her preference was to continue with this care. However, the scheduling for the carers is based on a prescribed day-of-the-week approach and not total hours. As she explained, this created a level of unnecessary inflexibility in the plan:
Tom had surgery seven weeks ago on both his legs. So a lot of my respite ended up being moved. Whereas I had it on Monday night and Sunday afternoon, it was now a lot more. I used a lot more respite because I needed extra help because he was in two casts. We have had to rejig and move days across and do lots of complicated things that the planner and the LAC have had to do... They have to move the funds. I used two different providers for respite. So if one worker is not available I have backup from another provider. They are both taking funds from that part of the plan. I actually ran out of Sundays so I have moved other days of the week over.[23]
2.31 Ms Jacqueline Pierce also informed the committee of the limitation of the disability respite services especially when compared to the resources provided in the aged sector:
An area of grave concern for me is detailed in the operational guidelines around supports for sustaining family carers in their role. That is a NDIS operational guideline—a public document...It talks about families getting as little as seven days a year of access to respite and a maximum of 28 days. Why would we actually think it is okay for people who work in an unpaid family carer role—often in a 24/7 capacity, and for an entire lifetime—to have anything less than four weeks off to recharge their batteries and enable them to continue in their family caring role for as long as they choose? In the aged care arena family carers are entitled to up to 63 days, or nine weeks, of government funded respite, and we all know that generally speaking family carers who care in the aged care space often have to provide care for a shorter period of time. Why are we telling family carers in the disability arena that they need less respite when they are supporting a loved one for an entire lifetime?[24]
2.32 Speaking to the committee the following day, Ms Gunn acknowledged that the lack of flexibility in participants' plans had left participants 'feeling very frustrated'.[25] She explained that the problems could be attributed to a combination of technical difficulties, a breakdown in the Agency's communication and, more broadly, the mindset of planners and the culture of the Agency (see paragraphs 2.48-2.51). In terms of the technical and communication difficulties, she told the committee:
Some of those errors have occurred purely because of numerical calculations of all of those mixes and there have then been errors with amendments when the person has said, 'Actually I don't want to do Saturday, I need to do Sunday.' We have had to change the plan to allow that because of the way the support lines have been implemented. The errors also reflect our failure to understand exactly what that person was previously accessing. Despite our ability to recently gather data, we did not have individualised data or a detailed understanding of what a person was accessing, particularly if they were accessing DOCS funded programs. Our planners would, in good faith, have a conversation with an individual and their family and, to a lesser extent, providers. Again, I will talk about what we need to do to address that. Then, when the person gets their plan and they say, 'But what about ... ?' and our planner was not even aware of that 'what about'—for example, 'the support I had on Sundays'—we have then gone through another conversation on a reasonable and necessary basis and made those amendments as well.
Importantly, though, many participants are seeing their plan as this dynamic relationship with the agency and that gives them the opportunity to say: 'Indeed, actually, I need something else in my plan; can I come back and adjust it?' That is an amendment; it is considered to be an error because the providers did not know about that previously. We are learning in these processes. Our system is very constraining. It has been incredibly frustrating for participants with that lack of flexibility and we will work with our national office to see what we can do about those individual support lines.[26]
The NDIA's IT system
2.33 On notice, the committee requested the Agency's response to these concerns with the lack of flexibility in participants' plans.[27]
2.34 The NDIA identified the information technology (IT) system as a major issue. Currently, it noted, planners need to add 'every possible individual support item to a participant's plan to ensure that they had flexibility to vary the days or times of day that they receive a service'. The Agency added that 'bundling of supports' will be introduced, allowing the participant to have the flexibility to purchase supports for any support item in these bundles.[28]
2.35 The NDIA informed the committee that it will resolve the problem of inflexibility of plans by introducing a system that allows the bundling of supports. It explained:
This means that the participant will have choice and control to purchase flexibly from all the support items in the bundle – not only the individual support items that have been included in the plan. The bundles that will be introduced which will allow flexibility within the bundle and across all flexible items in the plan include personal care, community access, interpreting and translating, and transport. If a planner sets up the plan using these bundles then the participant has flexibility to purchase supports for any support item in these bundles. An employment group has been set up which is fixed, meaning that the participant has flexibility to purchase any supports in the employment bundle but cannot choose to purchase other supports outside the employment supports. The flexibility is limited to employment and related items as this is an investment by the NDIA in the participant’s future employability.[29]
2.36 Certainly, participants and providers in the Barwon trial site also recognised the shortcomings of the IT system. Ms Krystyna Croft, whose 30 year old son has an NDIS plan, told the committee that the system 'seems very clunky' and added: 'One day I can see my son's full plan on the portal and the next day I can't'.[30] Matters relating to the service provider portal in the Barwon trial site are noted below.
2.37 The problems with the NDIA's IT system generally are discussed in chapter 6 of the report.
Participants' problems with transition: ISPs and the 'no disadvantage test'
2.38 The Victorian Government introduced Individualised Support Packages (ISPs) as a new way of funding people with disability. ISPs allocate funds to a person to meet their disability-related support needs. The Victorian Department of Human Services explains that ISPs enable people with a disability to 'direct the planning process to the greatest extent possible and make their own choices about how they wish to live their life'.[31] There are a limited number of ISPs and a very long waiting list.
2.39 In the Intergovernmental Agreement (IGA) for the NDIS launch, the Council of Australian Governments committed to provide continuity of support to people with disability currently receiving services to ensure that they are not disadvantaged in the transition to the NDIS. The IGA explains that where the NDIS takes on responsibility for providing continuity of supports for a person, 'the Agency will work with the person to develop a transition strategy to ensure no disadvantage in a person's outcomes'. It further clarifies that the supports provided by the NDIS will enable the person to achieve 'at least the same level of social and economic participation (or undertake the same range of activities) as enabled by their previously provided support'.[32]
2.40 Some participants and their carers (and even service providers) complained that they were experiencing difficulties making the transition from an ISP with the Victorian Department to a plan under the NDIS. These complaints had various dimensions.
2.41 Ms Vanda Fear, whose son Paul had an existing state funded ISP, was particularly critical of the process to transition people to the NDIS. In a written statement to the committee, she outlined her concerns:
We had previously been advised by many people associated with the NDIA that the transition for people from state-funded to NDIA supports, particularly in cases where things were working well would involve a 'light-touch' review in the first instance and a fuller review 12 months down the track. In our case nothing could have been further from the truth our lives were completely turned upside down in January 2014 and the stress for all of us has been enormous.[33]
2.42 Ms Fear told the committee at the hearing in Geelong of her concerns with the disability health interface. She argued that this interface 'is going to be critical for people with high and complex disability medical needs like Paul's' and added:
...we are living the reality that health do not fund much of what my son requires, which is why I have always received funding for medical health items related to my son's severe ABI through the ABI Slow to Recover program and then via his DHS ISP. The NDIA are not funding many of these things now, leaving my son at risk.[34]
2.43 Ms Fear told the committee that they are currently on the sixth iteration of Paul's NDIS plan. In her view, given her son's higher needs, this process risked breaching the 'no disadvantage test'. As she explained:
We were told that if you had an existing ISP you would not be disadvantaged in any way by this scheme coming in. Our son's package has been absolutely torn apart. Not everybody has higher health needs as well as a disability, as our son has. The argy-bargy that is going on between health and disability has put our son at risk so badly...We have been told that they do not fund it, but we have been told neither does anybody else. We did not get it funded by anybody. We had to try everywhere and get it from DHS, because there was nobody else in Victoria who could pay for it. But now we have been told that it is not going to be paid.[35]
2.44 Ms Fear noted that her son had 'the best therapist in Geelong', but that in moving to the NDIS, 'we have to fight now to keep our therapy component'. She explained that in the transition process, Paul was required to undergo an independent therapy assessment at significant cost:
It is now $164 an hour, plus travel and, in some circumstances, it is double that to get that person out to our home for one hour—over $300 for an hour! It used to be $80.
...
With respect to keeping even the level of therapist that we have currently, the cost has gone through the roof. Our plan has been decimated. We have a lot less supports now and it is costing a lot more. I do not understand it and I do not think it is viable to roll the scheme out like it is.[36]
2.45 Mr Stone of VALID put his frustration with the transition process in the following terms:
Our organisation has sat on representative bodies—with NDS [National Disability Services] and carers and other organisations—and collaboratively designed policies and guidelines. We sat around for 15 years developing principles around individualised funding—the ISP guidelines. I can proudly say as a Victorian that we had the best model, the best system, for ISPs in Australia if not in the world. Yet we have seen all of that experience and know-how ignored in these processes. It just does not make sense to me.[37]
2.46 Mr Alf Francett of Ermha, a Barwon-based community organisation supporting people experiencing the effects of a mental illness, told the committee that whereas ISPs offered holistic support for people with disability, NDIS plans are by comparison quite limited. He told the committee that in terms of the NDIS:
...if someone has got a forensic issue and has got a dual disability or a disability, they will fund the disability but they will not fund the forensic component of it because they believe they have got nothing to do with this disability, that that is all to do with the justice department and you need to get the funding from the justice department for that.
To say we will fund his disability but we won't fund what he does in the forensic component—even though he is on a first-name basis with the police and also the court system—makes it really challenging because the justice department will not fund it and the NDIA are saying it is not their area to fund.
...
Unlike the ISPs it is not a holistic approach. The ISPs looked at the whole person.[38]
2.47 The NDIA told the committee in an answer to a question on notice that the planning process considers a participant's existing supports prior to transitioning into the NDIS. The Agency informed the committee that it has identified some services that are currently funded through programs transitioning into the NDIA which are not generally funded by the Scheme and added:
In these situations the NDIA can fund the supports for a transitional period while the NDIA works with the participant to build their capacity to provide these supports for themselves or identify more appropriate sources of this assistance.[39]
The culture of the NDIA
2.48 The NDIS reflects broad-based community values and support and should evolve through the influence of community participation and involvement. The committee was concerned, therefore, to hear some participants' and service providers' views about the top-down and unresponsive culture of the NDIA. For example, Mr Stone told the committee:
We have all fought so hard to have a system that actually responds to the needs and interests of people with disability and their families and one that actually respects their commitment. The last thing we need is a model which imposes from Canberra or from Geelong any remote form of decision making on behalf of people with disability, but that is what we are getting. It is a Centrelink-type mentality on many fronts, and it just needn't be that way.[40]
2.49 Mr Stone also noted that the NDIA and the Australian Government had not conducted proper tendering processes:
...over the last 12 months, we fought to get capacity building funding for people with disability and their families. It was finally announced two weeks ago that $21 million to $22 million would be put into capacity building. That same tender process alludes to the setting up of a national non-government body to mentor and support disability support organisations for people with disability and their families, and the process of nominating such a national body is not open to tender. I think DSS is negotiating with a single body, without competition, without transparency and without any advice to the sector on the process for nominating such a group. To me, that is just wrong and it sets up a culture that we can frankly do without.[41]
2.50 The committee received complaints from several witnesses in Geelong about the slow response time of the Agency to requests for information and responses to complaints. Ms Gunn herself was quite candid about the need for the NDIA to improve in this area:
It is something that we need to get better at. We have put a particular focus since I arrived on trying to clear that backlog. We have complaints about complaints that did not get responded to, and I take that very seriously. In our defence, we have multiple IT systems that are designed to support us to do this work. They do not integrate or talk to each other. Our processes are not as rigorous as they should be, and we are very conscious of that. We are working to address that.[42]
2.51 The mindset of some of NDIA's planners, and the perceived culture of the organisation, is also reflected in what some perceive to be highly bureaucratic processes. Ms Knight expressed strong concerns with the way the Agency had requested that her son re-establish his disability. She explained that the requirement of re-filling a form to verify his disability left her feeling 'so patronised and demeaned'.[43] However, as this and subsequent chapters of this report state, the committee also received evidence from participants and carers of their very positive experience with NDIA planners.
The composition of NDIA staff
2.52 Some witnesses highlighted that the mindset of planners is strongly influenced by their background and previous experience and training. Mr Steven Hurd, a participant in the Scheme and an employee in a disability agency in the Geelong region, argued that there is a fundamental issue with the composition of NDIA staff:
...[W]hen it gets handed to the bureaucrats we get the same people doing the same things repeatedly. It is like a continuous cycle. The old system was bad. We have this great reform and we are going to change it. And who do they employ to change it? The people from the old system, which was bad... I have worked with people who work in this area and they are fantastic people. They are not poor characters, but they simply do not have the experience, knowledge, understanding and level of empathy to be able to make accurate decisions that are going to impact on the lives of people with disabilities, and carers.[44]
2.53 The committee took similar evidence from providers where witnesses drew the committee's attention to the composition of NDIA staff and also their expertise. Mr Rodney Harris, the CEO of Motor Neurone Disease Victoria, spoke about the generalist skill set of any of the NDIA staff:
It is with respect to the staff that have been recruited by the NDIA. They are generalist staff, which means they have excellent knowledge of a broad range of most common disabilities and the service needs of those clients. But they have little or no knowledge of the lower incidence, more complex diseases. We have planners who say, 'We are going to buy an electric wheelchair for that person because their average life expectancy on this letter from a doctor is five years and it is cheaper for us to do that,' but we know that average life expectancy across the last 30 years is about 27 months. To spend $15,000 on an electric wheelchair versus $6,000 to rent it for two years is not a good business decision for the NDIA, let alone common sense.[45]
2.54 Mr Hurd also emphasised the need to include more people with a disability into key decision making roles in all levels of the NDIA:
There really needs to be some real proactivity about getting people with disabilities into these agencies as client liaison officers, as capacity builders, and as people who can liaise with the community and talk to them and feed that back in to the planners and senior bureaucrats. Also, you need those people to be at a fairly senior level so that those bridges can be built. They should be people with disabilities and carers. There are more carers participating than people with disabilities. If women were told that 80 per cent of the people in the Office of Women's Affairs were going to be men, there would be a riot. Yet we people with disabilities have to live with that all the time. I am sure women in the audience and on the committee will understand the frustration people are feeling in this regard.[46]
Table 2.4: NDIA staff numbers and former employers*
|
Number
|
%
|
Former employer
|
|
91
|
60
|
Federal Government
|
|
18
|
12
|
State Government
|
|
42
|
28
|
Private Sector /Non-Government Organisation
|
|
151
|
100
|
Total Employees
|
* The table represents the previous employment areas for staff recruitment by National Office during the past 12 months.
Source: Response to committee request for information, National Disability Insurance Agency, received 26 June 2014.
2.55 On notice, the NDIA was asked if it could provide a breakdown of its current employees' previous employers and the number with a disability. Table 2.4 (above) shows that 60 per cent of NDIA staff were previously employed by the federal government. The NDIA also provided data showing that 11 per cent of its employees identify as having a disability. Within the trial sites, 12.3 per cent of NDIA employees identified as having a disability.[47] The committee discusses this matter further in chapter 6.
Problems with transport—participants
2.56 In the Barwon region, as in in the other trial sites, the issue of transport arose on several occasions as a matter of some difficulty for both participants and service providers. Mrs Jayne Crouch, a carer of a 21 year old daughter with Down syndrome, a 15 year old son with autism and a husband recovering from stroke, told the committee of her concerns with the mobility allowance:
My daughter got mobility allowance. The mobility allowance has now been rescinded. It comes under the NDIA. Initially, they were insisting that she use taxis. They have now agreed that they will fund for so many cents per kilometre. But this does not seem to be equal over all families or all services. Also, under the old system of mobility I was given a certain sum of money—or she was given a set sum of money—and that was it. Once you were approved you got that money every fortnight. I have to now put in a request for payment every month. In a family that is very busy, that is another heap of paperwork that I am supposed to do. I am also supposed to keep a log of everywhere I drive her. How practical is it for me to get in the car every morning with two people who have a disability, sit down and read my odometer and then discard the kilometres that it took to take my son to school so that I am only getting the right kilometres for her and then take off the kilometres, if I happen to stop and get an apple or something on the way? It is a very impractical system. And who is going to be reading all of that paperwork at the other end? It is creating a paper dragon.[48]
2.57 Ms Croft questioned whether participants should be encouraged to use a taxi as their prime mode of transport. She argued that as a result of the NDIA's focus on taxis:
[M]y son misses out on activities because the taxi does not come to pick him up because we don't have enough. So we need to build some flexibility into the transport types of funding.[49]
Problems with transport—service providers
2.58 The committee also heard of a range of concerns from service providers in the Barwon region. One of the most concerning related to administrative problems with the taxi industry which is faced with adjusting to a system where individuals pay for transport via the NDIA. Mr Peter Valentine, the Chief Executive Officer of the Geelong Taxi Network, told the committee that presently, it was not possible to dispatch a taxi for multiple transport users, which was clearly necessary under the NDIS. He argued: 'If we allow people to travel individually all of the time, we can see that those costs will blow out hugely and, in addition to that, it causes huge bottlenecks at the respective areas where we drop off or pick up if we have too many cars in the one area'.[50]
2.59 Mr Valentine also noted that a participant's plans are received by the planner far too late, which causes a range of problems. First, there will have been inadequate discussion with the planner as to what steps should be taken to speak to a transport provider. As a consequence:
We carried the finance debt for six months before we were able to get one stick of payment. The point here is not to do with the finance but to do with the organisation, because at that point in time we had already invoiced other service providers, such as some who have already spoken today. They may have already paid. We get a plan that is backdated two or three months, and there is a lot of messing around and toing and froing to try and identify those individual trips and then credit the actual people or the organisations.
We are told that we could have 2,000 people, for example, in the space of a couple of years under this program. If they travel morning and night five days a week, that is 20,000 individual entries for a little company like ours—although we are the largest urban company in Victoria, with 150 cabs and 589 drivers. I am totally scared, unless we get it right down here, about what will happen when it hits a capital city.[51]
2.60 Mr Valentine also had concerns about the NDIA's service provider portal and in particular, his company's experience with the low acceptance rate of entries into the Agency's computer system. He argued that when entering participants' details into the portal, roughly a third will not be able to be entered, whether the information is incorrect or does not match the NDIA's information. Another third will go into the system but will not be accepted by the system. And the final one-third does get accepted, although even a few of these require re-entering and lengthy correction process.
2.61 Mr Valentine also noted that a large number of accounts have not been put in—as many as 20–30 per cent.[52]
2.62 A further concern of Geelong Taxi Network is that operators struggle to identify NDIS customers. The driver is often not able to identify whether a person is, or is not an NDIS client. Mr Valentine also told the committee of the potential to abuse the system:
...if there is a person who lives next door to an NDIS person, it can quite easily lead to abuse of the account. The person next door phones up. He says: 'I'm Charlie Brown. I'm from the NDIS and I wish to go to XYZ destination.' The car pulls up. It pulls up out the front. He walks in. He gets into the car. The account gets charged to NDIS. There is no accountability for any client in that respect. There is no linking to the MPTP [Multi Purpose Taxi Program] card system. So these are the issues that we believe should be addressed in order to tighten the system up and also give our dispatchers more fluency for their dispatch.[53]
Service providers and the costs of the fee-for-service model
2.63 The committee also heard from Barwon service providers about the challenge of moving from a block funding system to one that relies on a fee-for-service. Mr Tony Still from St Laurence Community Support in Lara rejected the notion that the NDIS represented a 'free market' for service providers:
We talk about a free market, but we are not a free market when the prices are set for us. Unlike other health providers, we do not have the ability to co-bill so we cannot provide upskilling for our staff and we also cannot provide the basic repairs for our buildings and all the other things that go with running a business.
We are not a free market when we cannot charge for no-shows, and with our clients there is always going to be a fairly highly [sic] number of no-shows. So if one of our buses turns up at somebody's house and they are not available at that time, we do not get paid.
So we are basically stuck between a free market, with all the restrictions that apply, and a government-run type of organisation, with those sorts of restrictions. The charity model in the past has always put the client at the forefront of the business model, and the providers in the Barwon trial site have done that and have attempted to do that right through this trial. It has been to the detriment of the providers. That is all I will say in this first instance. But the premise that we are a free market is certainly not true at this point.[54]
2.64 Other providers in the Barwon trial echoed this sentiment. Ms Libby Mears, Chief Executive Officer of Leisure Networks, told the committee that the price set for some services is simply too low, which acts as a disincentive for providers to innovate. She gave the following example:
The social and community participation rate of around $34.50 an hour is low. It is lower than what DHS used to fund service providers for connecting people into community activities. The same service in South Australia is $40 an hour. So we have got two services that are the same but with different rates. That is low. When you are making a loss—and all providers are making a loss on that—you do get a bit risk averse around innovation and the opportunity to be creative. And that is a very critical area. So, when the free market arrives, I expect that that rate will need to rise, but some innovation will come with it as well.[55]
2.65 Mrs Rosemary Malone, the Chief Executive Officer of Gateway Support Services, agreed with Ms Mears' comments on the rate being too low. She also advised the committee that the previous week, a decision was made to stop taking new NDIS clients.[56]
2.66 The inability of service providers to charge for no-shows was confirmed in a response to a question on notice from the NDIA and is also in NDIA's public documentation.[57]
2.67 Mr Still noted that service providers are expected to make the transition to a fee-for-service model 'without the necessary support and without essential information from NDIS'. He explained that most providers in the Barwon area are small businesses which do not have the resources or the expertise to make the transition to a fee-for-service model within the expected timeframe.[58]
2.68 The committee notes that many service providers in the Barwon site, as in other sites, rely heavily on fundraising and other philanthropic donations. The Motor Neurone Disease Association of Victoria told the committee that even under the NDIS, 80 per cent of its funding will come through fundraising (see also chapter four).
Cross subsidising and fee gouging
2.69 The committee also acknowledges that service providers that are operating wholly within a trial site (or sites) face a quicker transition to a fee-for-service model than those with operations outside the trial sites. For example, Victorian service providers operating not only in Barwon but across the State can continue receiving block funding, while smaller NGOs operating only in Barwon cannot. Larger, broader-based NGOs can cross-subsidise their operation should there be financial losses in making the transition to a fee-for-service model in the trial site. Small NGOs, such as the Geelong Mood Support Group, are unable to do this.
2.70 Mrs Malone, made the additional point about the capacity of larger NGOs to cross-subsidise their operations if they were state based:
The other comment I would make is that there is actually a disadvantage in being a Barwon provider, a regional provider. If you are a state-wide provider, all the rest of your funding across the state continues to be stable, block funded and fully funded whereas we are dealing with multiple issues.[59]
2.71 This issue of cross-subsidisation, and the committee's deliberations on the matter, are discussed at the end of chapter 5 and again in the report's conclusions.
2.72 DHS responded:
...the issues around agencies being concerned about their viability, their cash flow, are conversations that agencies are raising with us and we are raising them on behalf of the NDIA. They are also raising them directly within NDIA. We have also engaged with the NDSV, the peak body provider across the state of Victoria, and we know that there is some work going on within NDSV about preparation for agencies.
There are a whole lot of conversations, but what I am hearing you say is that it has been quite compelling in terms of the number of agencies that are saying that they are concerned about viability and also access to community based services. It is something that we obviously need to listen to, talk to our colleagues in NDIA and understand what other things may need to be looked at.[60]
2.73 While the issues relating to the financial viability of service providers should not be downplayed, the committee also received evidence in Geelong that there is scope for service providers to take advantage of the NDIS to fee gouge. Ms Amanda Samek, a participant in the NDIS, relayed her experience:
A lady here spoke earlier about how her physio went up to $800. I had quotes done for my decking in the backyard. Being a bull at a gate, I rang the council and asked them to send someone out to give me a quote. I then had to hand the quote to the NDIA. The council gave me the quote and the NDIA said, 'Yes, that's fine. You can have that done.' I rang the council back to book in to have the job done. I said, 'The NDIA said that is fine.' The woman at the council said, 'Hang on a minute, you didn't mention the NDIA when you booked the quote.' I said, 'That doesn't make any difference, does it?' She said, 'It makes a big difference.' I said, 'Why is that?' She said, 'Because there is a different labour fee.' I said, 'Can you give me the proper quote, then?' She sent it out, and it was more than double the price.
...
As soon as you mention the NDIA, it is like saying it is a wedding cake, not a normal cake; it just goes through the roof, so I am self managing that too. Every time I go to the physio, I give them the receipt. The NDIA put the money in my account first for about three or four visits and I send them the receipts. I have always got a surplus in there to pay for regular visits and it keeps it at a regular price. I thought that might help other people because as soon as you mention the NDIA, it just goes through the roof.[61]
Incorrect plans
2.74 An area of potentially significant expense for service providers—in terms of both time and money—is the task of correcting errors in NDIA's plans. Mr Still estimated that St Laurence has had to spend well over $500,000 to become NDIS ready. It had employed 'more than four staff' to examine the plans provided from the NDIA to determine whether they are correct and whether they are financially viable. He estimated that 80 per cent of the plans are incorrect and observed that with the speed that the NDIS prepares the plans, there is 'very little consistency in the plans'.[62] Mr Still also noted that while the cost of many of its participants' plans had gone down, St Laurence has had to make some difficult decisions and advise participants that it can no longer provide the service.[63]
2.75 Other providers in the Barwon trial concurred that many NDIA plans required amendments which resulted in significant extra unpaid work and costs for service providers. Ms Malone of Gateway Support Services told the committee:
For us, in our respite and recreation programs we have had a large amount of unfunded work. Tony talked about 80 per cent. I asked our staff and they said, with our respite and rec programs, probably 90 per cent of the plans have required further discussion because the rates during the week, on Friday night, on Saturday, on Sunday—are all different and it also depends on whether it is a group or an individual program. And if families say, 'I would like to use some of this and some of that', and it is not in their plan, there is a process of going backwards and forwards so that the plan actually has the things in it that they need. It might be that they have got community participation but there is no travel for them to actually go somewhere. So we have spent a large amount of time doing unfunded work to sort out our plans.[64]
2.76 The committee asked for more detail on the nature of the errors in plans. Mr Still explained:
There are the general mathematical errors where four days at six hours is apparently 30 hours over a week. There are plans that do not add up as far as the interventions are concerned. The plans can be very, very detailed if a person is using a number of different providers, so we are trying to ascertain when we can put the person into a service. The plans can be missing things like transport or services and support that the person has had in the past. So we have a number of people going through those plans with a fine toothcomb.[65]
2.77 The committee emphasises that service providers are not compensated for the additional effort they undertake to correct NDIA plans. The committee notes that many registered service providers have been incurring costs in fixing the NDIA's administrative errors in plans. The committee believes that this should be a responsibility of the Agency.
2.78 In terms of what constitutes a good plan, Mr Still emphasised the importance of a plan meeting the needs of the consumer long term by way of the service and support that they need. He noted that a good plan is one that recognises the value of early intervention in certain areas, where a little bit more now saves further down the track.
2.79 The committee also asked St Laurence to elaborate on why a plan might be considered 'financially unviable'. Mr Still responded:
Financially unviable is where we will be given a plan for 43 weeks on the basis of holidays and various different times when the consumer does not think they will be available, according to NDIS. We still pay our staff 52 weeks of the year, so on that basis a $22.70-odd an hour plan will not be viable.[66]
Mental health and the financial viability of service providers
2.80 The committee understands that the inclusion of people with mental health illnesses into the NDIS has yet to be settled and remains a matter of immediate and significant concern for the NDIA and federal and state governments. Two key issues were raised at the Geelong public hearing which will be revisited throughout this report. The first is how those with a mental illness will be assessed in terms of eligibility for the NDIS (Tier 3), and what supports will be provided for those who are found to be ineligible and fall into Tier 2. The second issue concerns the end of block funding and how this will affect the financial viability of small organisations that provide mental health support services.
2.81 In terms of eligibility for mental health access to NDIS, Mr Reid Maxwell of the Geelong Mood Support Centre expressed concern at the NDIS criteria of a 'permanent mental health issue' and the process through which a person is assessed for a package of supports. He argued:
We certainly have an issue with the criteria of someone having a permanent mental health issue. It was something that was probably thought about in the 1980s but right now the permanency of mental illness is considered something that does not need to be talked about and, unfortunately, people who have mental health issues, if they do go to the NDIA to get assessed, have a great fear of rejection...They have a great sense of being unable to describe their functionality to someone who is either a planner or an assessor or someone else altogether.
The sense with mental illness is that it is of such an episodic nature. You can have individuals who can do all the things that are on the form at particular times during the year and then at other times of the year they can do nothing on the form. I have seen a number of forms filled out by GPs or by psychiatrists that say, 'This person has no functional deficits.' Their deficits are around emotion and emotionality. I think the NDIA has really missed its mark on trying to encapsulate mental illness and the types of supports that people with a mental illness need. It is not about getting people to do 'human doings'; we are trying to find individual places and responsibilities within our community where they can have a role.[67]
2.82 Mr Maxwell also argued that the NDIA needs to be more focussed on ensuring that a person with mental illness 'can take control of their lives, can have a role to play in the community and can put back knowledge into the community'.[68] He called for greater incentives to encourage people to rejoin society and finish their program of supports.
2.83 The committee notes that Mr Eddie Bartnik has been appointed as a strategic adviser to the NDIA to address the issue of Tier 2 supports, and to identify the type of supports available to people with a mental illness.[69] Moreover, the committee draws attention to the lack of a fully-developed Tier 2 strategy and recognises that as a consequence, many people feel vulnerable and at risk. This report recommends that action is needed—through the Council of Australian Governments—on a Tier 2 strategy as a matter of priority (see chapter 6).
2.84 The second issue concerning mental health services under the NDIS relates to the viability of the providers. The committee heard concerns that small mental health support service providers, which had previously attracted block funding, would not be financially viable under a system where funding is on the basis of individuals paying from their NDIS packages. Mr Felix Firgaira, a client of the Geelong Mood Support Group, put the dilemma as follows:
They used to get funding for the whole of the group and now the funding needs to be through individuals who get some sort of a package and then the funding will be made according to the number of people. If they had 100 members that were part of the group before, now they have got to try and get 100 people to apply for a package and some of those 100 may not qualify. There may be some whose disability is not bad enough according to their doctor.[70]
2.85 Mr Maxwell told the committee that in addition to this broad transitional issue, the Mood Support Centre, as a registered service provider of the NDIS, is not able to access any of the $121 million of funding for Disability Support Organisations (DSOs).[71] The committee queries why the Geelong Mood Support Centre is not eligible for DSO funding and seeks clarification from the NDIA as to why this is the case.
2.86 At the public hearing on 15 April 2014, the committee asked the Victorian Government to respond to concerns that organisations, such as mental health providers, that are not funded to provide people with individualised types of supports, will be lost in the transition to the NDIS. Ms Anne Congleton from DHS appeared to doubt whether these organisations would be lost:
Some of it is about the interactions with the mental health agencies and, as they are looking at phasing coming through, the importance of upping the understanding and the discussions that are going on. Sometimes it is about real issues and sometimes it is about the uncertainty that exists for them about changes and what may be. From a local point of view, that is in our sights in terms of making sure that we are working with the mental health providers as closely as possible to understand what it may mean and what it will mean.[72]
2.87 DHS also told the committee that the provision of mood support services under the NDIS is 'a complex issue and one that we are still trying to work towards over a full scheme'. It noted that DHS, the Commonwealth and other state governments are currently working on how to address these advocacy and support issues.[73]
2.88 In June 2014, the committee received correspondence from Psychiatric Disability Services of Victoria, the peak body for community managed mental health services in Victoria. It noted that clients and families were reporting negative experiences about the NDIS planning process, particularly the lack of time in this process to appropriately identify and meet needs. It highlighted the following issues:
- the price of supports for people with mental illness are inadequate;
- the rest of Victoria is funded at a different cost under the reform, putting Barwon services at a disadvantage;[74]
- the financial burden on services in the transition process is significant, with no allocation of resources;
- there is a lack of clarity around how the needs of Tier 2 clients will be met;
- only face-to-face time is funded, with no recognition of the additional time required for complex case support;
- there is a lack of understanding and recognition of workers' skills and qualifications, and what is needed in the workforce to provide effective support for people with mental illness;
- there is an unrealistic expectation of the capacity of services to be able to meet demand;
- the timeframes for funding and client transition are in conflict impacting on service viability; and
- there is lack of support for services in the transition and for their input into development and review of the process.[75]
Relationship between the NDIA and providers
2.89 Engagement with peak groups and service providers is critical to the success of the NDIS. On this matter, the committee heard evidence from the Motor Neurone Disease Association at the Geelong hearing:
We have made a number of suggestions to the NDIA. One is about bundling for people who have a progressive neurological condition, whereby they should automatically have a small selection of the core needs that we know every person, for example with motor neurone disease, has—some funds to rent equipment; some funds for complex case coordination; and some funds for, for example, respite care. The proposal was put to the NDIA and whilst it was received enthusiastically at the top, it went down like a lead balloon the further through the organisation we went. But we still believe that the NDIA is not drawing on the skills, knowledge and experience of the organisations particularly in this area. We tend to find that we have been treated like the enemy. Communication was very poor. In the last two months there has been a remarkable turnaround. I think the second quarter report has actually raised the issue of more effective use of resources that exist in the community and being able to actually return emails and provide information when it is requested.[76]
2.90 The Chief Executive of the Association, Mr Rodney Harris, told the committee that automatically bundling supports for people with Motor Neurone Disease would take the NDIA less than three hours to complete a first-up plan. He added: 'It is a business decision. It is a sensible business decision and a cost-effective decision that we are putting to them'.[77]
2.91 At the time of giving evidence, some Barwon-based service providers shared concerns that the NDIA had failed to strategically engage service providers to date. Ms Libby Mears, Chief Executive Officer of Leisure Networks stated:
Although engaging at the operational level is important, there are probably more opportunities for providers to engage to inform some of the strategic directions so that our experiences might improve and so that we are actually all part of moving forward together. I will leave it at that. I think the providers are probably not as engaged as they could be. There are a lot of day-to-day challenges, but in talking about strategic opportunities, I think that would be really valuable.[78]
2.92 The committee notes that the NDIA is now moving to greater engagement with the disability sector by hosting regular forums to hear the experiences of participants and providers.[79]
Housing issues
2.93 A challenge common to all trial sites is the issue of housing and in particular, the high level of unmet need for a range of different housing options. The committee emphasises that housing for people with disability has been a significant issue for some time. It has in no way become a problem because of the NDIS. Indeed, the NDIS is an opportunity for governments to fix the problem. This will require strong leadership from the federal government (see chapter 6).
2.94 The transition to the NDIS is occurring at a time when state governments are 'deinstitutionalising' their disability accommodation centres. In practical terms, this means that people currently within these centres will be moved into supported accommodation within the community. In Victoria, the state-run centres are the Colanda and Sandhurst Residential Centres. As shown in Table 2.2 at the beginning of this chapter, residents of Colanda will be brought into the NDIS in September 2014.
2.95 At the Geelong hearing on 14 April, housing was raised in various contexts. All the issues related to the capacity of persons with disability to find appropriate supported accommodation in the community. Miss Kirrily Hayward, a 26 year old currently residing in an aged care facility in Geelong, told the committee:
My primary condition is spina bifida, L4-5, and wheelchair bound as a result. I am fairly independent and can do most things myself. I am fiercely outgoing and very active. But the thing that is holding me back is my current health condition and the fact that I am residing in an aged-care facility to receive treatment. The issue I find the hardest has been trying to transition out of aged-care and find the facilities for me. There are only six supported accommodation facilities within the Geelong and Surf Coast region. I have also noted that I fall into the nice little gap where I am fiercely independent, fiercely outgoing and can look after most aspects of my self-care but I still need that extra bit of psychosocial support, medical care plus a little attendant care support, and I have trouble when I am reviewed or assessed for any such supported accommodation because, realistically, as an entity I can only tick one or two of those boxes. I do not fit all the criteria. Hence, the reason that it has taken me so long to find appropriate accommodation to fit my needs.[80]
2.96 DHS has noted that the Younger People in Residential Aged Care initiative concluded in 2011. Over five years, the initiative delivered:
- 104 new, purpose-built accommodation and support places at 22 sites;
- allowed 50 persons to remain in their homes or other private accommodation; and
- delivered 70 individual support packages to enhance the quality of life for younger people still living in residential aged care services.[81]
2.97 DHS noted that younger people with disability living in or at risk of entering residential aged care have priority status on the DSR for access to individualised support packages and/or vacancies within supported accommodation when they become available.[82] The issue of young people living in residential aged-care is revisited in chapter 4 of this report.
2.98 Ms Croft had a different accommodation problem. As she explained:
I have a 30-year-old son who suffers from significant cognitive impairment ...We are completely stymied in Victoria, over developing accommodation, because of fire sprinklers. As I understand it, we have the most stringent regulations of any state. My son does not need to have someone leaning over his shoulder all the time, but he does require to be supervised, which means he needs to have a sleep-over. Nobody can give me the exact answer why—it may lie in the Building Code. I have explored the DHS regulations. I believe that applies to houses funded and managed by DHS, but it may not apply where we have got Commonwealth funding.
I, with a group of people, was looking to rent a house. We thought it would be quite easy: 'Let's go and rent a house. We'll have four bedrooms. We'll put three participants in, and the fourth bedroom will be for a sleep-over.' 'Oh, where is your fire sprinkler? You're not going to get a landlord to put in a fire sprinkler, are you?' A housing association said, 'Not a problem. We're providing accommodation for your son; that's all we're doing.' But now they are getting a bit nervous because it is morphing into a workplace—as well as needing sprinklers. We went to a service provider who initially said 'That's quite easy, we'll provide supports. Oh, no fire sprinklers!' So they are pulling out.
The only possible way we might be able to do this is if we employ the support workers ourselves. Frankly, I am not going to risk my assets to do that, nor do I want to be in a position where I am working full time to support my son. The whole point is for him to become independent. He is going to be less of a liability on the state system—and I use that broadly. If he can morph into independent accommodation, we can look at electronic surveillance; down the track, there are a whole lot of things we can start to look at. But, if it remains in the position he is in now, he is going to be a very big liability to the system.[83]
2.99 Ms Croft told the committee that what is needed to resolve the current situation is collaboration between all tiers of government and housing associations. She emphasised that people with disability have different accommodation needs and it is not as simple as pooling resources and moving in.[84]
Committee view
2.100 This chapter has outlined the main challenges and achievements of the Barwon trial site as presented to the committee on 14 and 15 April 2014 in Geelong. As noted at the outset, it is by no means a comprehensive account but it has identified those matters that witnesses thought—in their experience—were the achievements and issues of most concern in the progress of the trial.
2.101 The committee itself has a number of concerns arising from the evidence that it heard in Geelong from participants and service providers. It has pursued these matters in questions to NDIA and DHS officials on 15 April 2014 (see Hansard transcript) and in written questions on notice to the NDIA (see Appendix 3) and DHS (see Appendix 5). The committee is pleased that at least on some of these issues, there has been greater progress.
2.102 Two themes developed in this chapter recur throughout this report. The first is the culture of the NDIA and its need to improve the format, style and responsiveness of its communications with participants, their families and service providers. For many people, the experience of participating in the NDIS was very positive. However, other evidence from the Barwon trial site indicates there is a need for the Agency to focus on the participant and carers, rather than prioritising compliance with processes over their needs.
2.103 The second issue relates to the long term development of the disability support sector in the Barwon region. The committee seeks the Agency's response on the issue of how much has been spent and committed from the NDIA's Sector Development Fund in Victoria. In particular, the committee seeks information on the cost of grants delivered, to whom and for what purpose.
2.104 These and several other themes identified in this and subsequent chapters will form a baseline for examination and reporting by this committee.
Navigation: Previous Page | Contents | Next Page