Background
2.1
The terms of reference for this inquiry reflect a proposal for life
insurers to have a greater role in providing rehabilitation and related health
services presently prohibited by the Health Insurance Act 1973. This
proposal was expressed in evidence by various members of the life insurance
industry, particularly the Financial Services Council (FSC).
2.2
In brief, the FSC posited that some Australians experience a gap in
their cover when seeking access to medical treatment in order to recover from
injury and return to work. Observing that this gap has negative repercussions
for the individual, for society, and for the economy more broadly, the FSC
argued that the life insurance industry is well-placed to address this problem
but is currently prevented from doing so. In addition, the FSC indicated that its
proposal would help address concerns about the financial sustainability of the
life insurance industry.
2.3
The FSC's proposal calls for amendments to primary and delegated legislation
that currently prohibit life insurers from providing benefits for worker
rehabilitation in certain circumstances. A representative of the FSC presented
the proposal in a positive light:
It's not every day that you see a convergence of the interests
of customers and private sector providers in relation to a public policy issue
which also contributes positive benefits to the Australian economy through
increased workforce participation and lower government health and welfare
expenditure.[1]
2.4
This chapter outlines the FSC's proposal and puts it in context, as
follows:
-
firstly, the problem that the proposal seeks to address;
-
secondly, the origins of the proposal; and
-
thirdly, the details of the proposal.
The problem that the proposal seeks to address
2.5
Currently, an injured person can receive assistance for medical
treatment from various sources. This includes benefits received under Medicare,
private health insurance, or other schemes such as workers compensation or
travel insurance.[2]
2.6 Despite these possible funding sources, the committee heard evidence
indicating that Australians can experience a gap in their coverage.[3]
This gap can arise in various circumstances, including where the injured
person:
-
has exhausted their Medicare benefits, or Medicare does not cover
the treatment they require;
-
does not have private health insurance, or their private health
insurance does not cover the treatment they require, or they have exhausted
their private health insurance coverage;
-
has exhausted benefits subject to statutory caps applying to
workers compensation or similar schemes; or
-
is unable to access other sources of cover, such as workers
compensation schemes, including because the injury did not take place at work.[4]
2.7
Even where an injured person is covered, it is possible that they will
experience delays in accessing treatment. This could be, for instance, due to
wait times in the public health system.[5]
2.8
The FSC cited research which illustrates that the longer a person spends
away from work, the less likely it is that they will return to work:
If a person is off work for:
-
20 days, the chance of ever getting back to work is 70 per cent;
-
45 days, the chance of ever getting back to work is 50 per cent;
-
70 days, the chance of ever getting back to work is 35 per cent.[6]
2.9
The FSC's Director of Policy and Global Markets,
Mr Allan Hansall, also referred to economic modelling (commissioned
by the FSC and some life insurers) to show how many people experience a gap in
coverage and could benefit from the proposal:
[R]eforms could provide benefits to a pool of up to 10,118
people a year. Of this pool, Cadence [Economics] conservatively estimates that
there are 1,379 people for whom early intervention would be beneficial and cost
effective, potentially rising to 3,600 under the research's high-side scenario.
It is thought an average of 87 people per year could be prevented from becoming
totally and permanently disabled as a result of receiving additional healthcare
intervention paid for by life insurance...Cadence's report estimates early
intervention could improve return to work times by five weeks, from 18 to 13
weeks.[7]
2.10
Mr Hansall told the committee that the FSC supports the proposal because
it is 'the right thing to do for our customers, to make sure that what we do
responds better for them and is more efficient'. However, he also acknowledged
that the proposal would save insurers money, because intervening early and
helping the policyholder return to work may reduce the need for larger payouts
down the track.[8]
2.11
On this latter point, the committee understands that the Australian
Prudential Regulation Authority (APRA) has identified prudential risks in the
life insurance industry.[9]
While life insurers were profitable between 2009 and 2016, this was primarily
driven by Individual Life Lump Sum business (which includes death cover,
trauma, and total and permanent disability insurance). Life insurers
experienced low returns and material losses in respect of individual disability
income insurance (also known as income protection insurance) and group lump sum
business.[10]
2.12
APRA provided the following chart, which shows life insurers' net profit
after tax in risk products, from 2010 to 2017:
Figure 2.1—Life insurers' net profit after tax in risk
products, 2010 to 2017
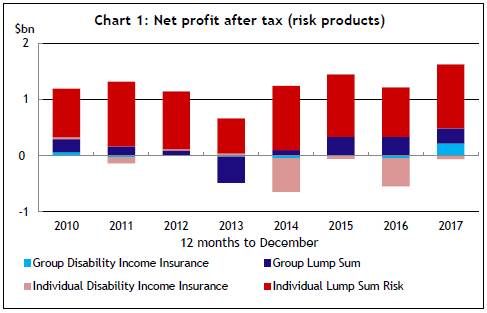
Source: Australian Prudential
Regulation Authority, Submission 10, p. 2.
2.13
APRA told the committee that there are a variety of factors driving
these losses, and the sustainability of the industry is an issue that APRA is
continuing to address. However, APRA said that the provision of 'early and
targeted rehabilitation and medical benefits to improve return to work rates
for [disability income insurance] policyholders' could help improve the
sustainability of the industry.[11]
2.14
Indeed, an FSC representative explained that the proposal is partly
intended to assist with the sustainability of the life insurance industry:
For insurers, the reform is also about reducing the cost of
income protection and total-and-permanent disability claims, and making these
policies more sustainable in the longer-term. This is beneficial for customers
and insurers because it reduces cost to the risk pool, which will be
transferred to all customers through cheaper insurance. It is also beneficial
for government and taxpayers because it helps reduce people relying on welfare
benefits.[12]
The origins of the proposal
2.15
The committee recently completed a substantial inquiry into the life
insurance industry.[13]
It presented its final report for that inquiry on the same day that this
inquiry was referred to the committee.[14]
2.16
In the committee's report on the life insurance industry, the Chair,
Mr Steve Irons MP, reflected on the nature of Australia's life
insurance industry:
The life insurance industry is a significant part of the
financial services sector in Australia. It has a noble purpose in providing
financial protection to policyholders in times of need and financial distress.
Despite this, there are sections of the industry that can and must do better in
delivering the protection they promise whilst remaining financially viable long
into the future.[15]
2.17
The committee made a total of 49 recommendations, many of which were
directed either at government or the life insurance industry itself. The committee's
report focussed on areas where 'substantial changes are required to ensure the
life insurance industry is held to account', namely:
-
effective consumer protections and industry codes of practice;
-
the transparency of remuneration, commissions, payments and fees;
-
the provision of advice in the best interests of consumers;
-
group life insurance arrangements that do not disadvantage
certain groups of consumers;
-
appropriate access to personal medical and genetic information;
and
-
fair claims handling practices.[16]
2.18
During the committee's inquiry into the life insurance industry, some
submitters drew attention to restrictions on life insurers' ability to pay
medical expenses and other benefits for worker rehabilitation. The FSC in
particular argued that these restrictions should be lifted, and put a proposal
that resembles the one being considered under the current inquiry.[17]
2.19
In its previous inquiry, the committee acknowledged the importance of
early intervention and measures that support worker rehabilitation. It also
noted that the detail of the FSC's proposal arrived fairly late in the inquiry,
so the committee did not have an opportunity to hear from other witnesses and
submitters about any potential unintended consequences. The committee made the
following recommendation:
The committee recommends that the Australian Government
conduct a thorough inquiry or consultation process before it progresses any
reforms relating to life insurers funding rehabilitation services, including
impacts on private health insurance, or Medicare, and any conflicts of interest
that may arise for an insurer vis-a-vis their customer and the most appropriate
care.[18]
2.20
During this inquiry, FSC representatives were asked whether the FSC was
in conversation with the government about advancing the FSC's proposal.
Mr Hansall of the FSC advised the committee he was not aware of any such
conversations.[19]
2.21
However, the Treasury informed the committee that last year the FSC
wrote to government outlining its proposal at a high level. The government saw
potential benefits and risks to the proposal, as the Treasury told the
committee:
From the government's perspective, it was really a case of:
'Well, this is an interesting issue. We can see that it's a complex issue. We
can see that there may be some gains.' I think the government made a decision
to refer the matter to this committee to see if it could dig up some
submissions and shed some light on more-detailed proposals from the industry in
terms of how it might work and how the regulation might work, given that it's
pretty complex, across life, super and health.[20]
The detail of the proposal
What are the current restrictions
on life insurers?
2.22
Life insurers currently offer a variety of continuous disability
policies. These include total and permanent disability insurance, income
protection insurance for temporary incapacity, and trauma or critical illness
benefits for specified illnesses, conditions or injuries.[21]
2.23
The FSC told the committee that life insurers routinely provide rehabilitation
services under these policies to help claimants recover from injury.[22]
Indeed, the committee understands that many life insurers are investing in in‑house
rehabilitation resources.[23]
2.24
While the current regulatory system allows life insurers to provide some
vocational rehabilitation services, it does not allow them, in certain
circumstances, to pay for medical treatment or therapy that could help
claimants return to work.[24]
As the FSC explained, life insurers are currently not permitted to:
...provide a benefit to a claimant under a continuous
disability policy for treatment costs where either a corresponding Medicare
benefit is payable or where the treatment is a hospital treatment or general
treatment (and is not otherwise excluded from the concept of a health insurance
business).
This restriction applies regardless of whether the Medicare
or Private Health Insurance benefit is exhausted, meaning that any gap in costs
after reimbursement under a private health insurance policy or receipt of a
Medicare benefit will not be able to be paid by the life insurer and will need
to be funded directly by the person receiving the treatment.[25]
2.25
The following table, which was provided by MetLife, distinguishes between
the benefits that, at the moment, life insurers are generally permitted and not
permitted to provide:
Table 2.1—Benefits that life
insurers are currently permitted and not permitted to provide
Benefits that are
generally
permitted |
Benefits that are
generally
not permitted |
| Lump sum payments for
total and permanent disability insurance |
Physiotherapy |
| Income replacement
payments |
Psychiatric treatment |
| Vocational guidance |
Psychological counselling |
| Occupational
rehabilitation |
Funding for surgery |
| Training support |
Any treatment that may be
a Medicare benefit |
| Referral to support
services (such as community based services) |
|
Source: MetLife, Submission
13, pp. 3–4.[26]
2.26
These restrictions are given effect by a range of legislation and subordinate
legislation, including (but not limited to) the:
-
Health Insurance Act 1973, including section 126;
-
Income Tax Assessment Act 1997, including
section 295.460.
-
Life Insurance Act 1995, including sections 9A and 234;
-
Private Health Insurance Act 2007, including
section 121-1;
-
Private Health Insurance (Health Insurance Business) Rules 2018,
including rule 16;
-
Private Health Insurance (Prudential Supervision) Act 2015,
including section 10;
-
Superannuation Industry (Supervision) Act 1993 including
section 62, and
-
Superannuation Industry (Supervision) Regulations 1994, including
regulation 4.07D.[27]
2.27
The FSC's proposal would reduce these restrictions, and its submission
provided some specific amendments to the above legislation and subordinate
legislation.[28]
How would the proposed system work?
2.28
The committee acknowledges that the proposal has not yet reached a stage
where specific legislative amendments have been drafted in bill form. It also
notes that the proposal has been presented by various members of the life
insurance industry and in various pieces of evidence. Nonetheless, it appears
that the key features of the proposal include the following:
-
In the first instance, an injured person would seek assistance
for rehabilitation from existing sources of cover, such as Medicare, private health
insurance, and workers compensation.[29]
-
A life insurer may provide assistance for a person's
rehabilitation if existing sources of cover are:[30]
-
insufficient (possibly because the relevant treatment is only
partially covered);
-
not immediately available (including 'where waiting times in the
public health system would result in an adverse return to work outcome');[31]
or
-
otherwise unavailable (possibly because the injured person is not
covered or has exhausted their coverage).
-
In cases where existing sources of assistance partially cover the
rehabilitation costs, the life insurer may pay the gap payment. In other cases,
the life insurer may cover the full cost.[32]
-
The injured person would need to hold a continuous disability
insurance policy in order to be offered rehabilitation assistance by a life
insurer.[33]
-
The life insurer would not offer to pay for medical treatments
for every customer. As the FSC stated, payments would be made at the life
insurer's discretion 'if it makes financial sense to do so'.[34]
The committee understands that this may refer to cases where the life insurer
considers that providing rehabilitation assistance would save it money in the
long run (for instance, by assisting an injured person to return to work the
insurer may avoid making larger payouts under income protection insurance down
the track).
-
The proposed payments would not be part of contracts with
customers, and provision of the payments would not appear in product disclosure
statements.[35]
-
Life insurers would be able to provide rehabilitation assistance
to an injured policyholder regardless of whether or not the injury was work‑related.[36]
-
Any assistance offered by a life insurer would be arranged
through the policyholder's treating physician with the policyholder's consent.[37]
However, the life insurer would also 'assess any ideas that are put to them
from the customer in partnership with their medical advisor'.[38]
As an FSC representative explained:
The GP would make the decision
about whether the treatment is appropriate and effective and will return the
person back to work earlier. An insurer will make the decision about whether
they will choose to pay for it.[39]
2.29
Mr Hansall of the FSC emphasised that this proposal 'is not about
life insurers providing private health insurance by the back door or stepping
in the way of existing workers compensation schemes'. Rather, the proposal
intends to provide additional, complementary support where that support would
help with the policyholder's recovery but is not available through other
coverage.[40]
2.30
MLC Life Insurance similarly clarified that the intention is for life
insurers to act as a 'supplementary funder' of medical treatments, which means
that 'any funding would be additive to existing health funding sources in a
limited range of circumstances'. These 'top up' payments would only be made if
both the following criteria are met:
- Where
it can be demonstrated that the planned medical service is reasonable and
necessary to the goal of restoring the customer to health and employment.
- Where
principal healthcare funders are constrained from funding the required services
due to regulation, timing of the availability of treatment (including health
system capacity issues), or, in the case of private health insurance, the
customer is not insured or has exhausted their benefits.[41]
2.31
The FSC also provided four overarching points about how the proposed
policy framework would operate:
- All
treatment the life insurer offers to pay for would be arranged through the
claimant's treating physician with the customer’s consent.
- Life
insurers will not coerce or pressure customers to seek treatment or return to
work.
- Life
insurers will not stop Income Protection (IP) or Total and Permanent Disability
(TPD) insurance payments merely because a customer refuses any treatment that
is offered.
- Decisions
and processes relating to an offer to pay for treatment would be subject to the
usual internal dispute resolution and external dispute resolution processes.[42]
2.32
In conclusion, Mr Hansall of the FSC told the committee that the
life insurance industry would, in consultation with government, 'ensure this
policy is ring-fenced by the proper consumer protections'. He strongly
recommended that any legislation passed to enact the proposal should also
provide for a review to be conducted three or five years after commencement.
The review would consider the effectiveness of the legislation as well as the
conduct of life insurers.[43]
Navigation: Previous Page | Contents | Next Page