Chapter 2
Key issues
2.1
This inquiry attracted a large volume of submissions and correspondence
from individuals who held serious concerns about the Social Services
Legislation Amendment (No Jab, No Pay) Bill 2015 (Bill). The majority of the
submitters were concerned about the Bill's measure to remove conscientious
objection as an exemption category for eligibility for social security
payments.
2.2
The key concerns raised by submitters and witnesses were:
-
efficacy of the Bill in increasing vaccination rates;
-
impact on disadvantaged families;
-
suitability of proposed exemption categories;
-
need for a vaccination injury compensation scheme;
-
impact on child care providers; and
-
accuracy of the Australian Childhood Immunisation Register data.
2.3
The committee also received some submissions that supported the proposed
measures, suggesting they would increase vaccination rates and improve public
health outcomes. For example, Friends of Science in Medicine stated in their
submission that the Bill is 'feasible, acceptable to the community, ethical and
legal.'[1]
Furthermore, The Parenthood, a group of 35,000 parent members said in their
submission that the Bill 'sends a strong signal to all parents that
vaccinations are necessary and safe'.[2]
2.4
The Department of Social Services (DSS) submitted that:
The Australian Government considers that immunisation is an
important health measure for children and their families as it is the safest
and most effective way of providing protection against diseases.[3]
Efficacy of increasing vaccination rates
2.5
A large number of submitters and witnesses raised questions as to
whether the Bill will achieve the desired result of increased vaccination
rates.[4]
2.6
The Explanatory Memorandum of the Bill states that savings of $508.3
million over the forward estimates are expected as a result of this Bill.[5]
Submitters said that the anticipated savings suggests that the Government
expects the Bill will not persuade some families to vaccinate resulting in a
reduction in social security payments.[6]
DSS told the committee they expect that in 2016–17 around 10, 000 families will
lose an average of $7,000 in child care payments and 75,000 families will lose
the FTB-A supplement, which is currently $726.35.[7]
Conscientious objectors
2.7
The Bill's proposed measures seek to address the growing rate of
conscientious objectors (COs) and the risk this poses to young children and the
broader community.[8]
2.8
The committee notes that the percentage of children registered as COs has
steadily increased from 0.23 per cent of total children in 1999 to 1.77 per cent
in 2014. This equated to 39,523 children in 2014.[9]
The Australian Medical Association (AMA) has expressed concern about the
growing rate of conscientious objection to vaccination in Australia.[10]
2.9
Vaccination rates for one and two year olds have remained steady between
89-92 per cent for more than a decade and for five year olds have increased
from 74 per cent in 2005 to 92 per cent in 2014.[11]
However, the AMA says this is below the recommended 95 per cent needed to
maintain herd immunity.[12]
Herd immunity helps to protect babies who are too young to be immunised as well
as the elderly and the immunocompromised, 'such as people undergoing cancer
treatment, transplants, or those with allergies to vaccine components'.[13]
2.10
Furthermore, evidence to the committee suggests that COs exist in
clusters across the country,[14]
and that the vaccination rates of the communities in which they reside are much
lower than the state or national average.[15]
The AMA submitted that these areas are more prone to outbreaks of vaccine preventable
diseases.[16]
Northern Rivers Vaccination Supporters is a community group from a region with
some of the lowest rates of immunisation nationally, such as the Byron Bay Shire
where the vaccination rate for 5 year olds in 2012–13 was 66.7 per cent.[17]
Their submission discussed the impact of low vaccination rates:
In the Northern Rivers the 'chink in the armour' is a perfect
storm of dense clusters of unvaccinated children congregating together in a
child care centre, putting the whole region at risk of subsequent outbreaks.
This is already happening, and we see this with frequent outbreaks of Pertussis
in our region. This has already proved fatal to those too young to be
vaccinated themselves.[18]
2.11
The committee received submissions from COs stating that the Bill will
not influence their decision to vaccinate.[19]
Furthermore, submitters argue that families who can afford to relinquish social
benefits will not be easily motivated to change their position as a result of
the Bill.[20]
2.12
Associate Professor Julie Leask, told the committee that about half of
all COs would be very difficult to influence.[21]
She said that for the other half (those who could be influenced) evidence
suggests that 'strategies that focus at the immunisation provider level are
very important'.[22]
DSS told the committee that the rate of objection to vaccination is expected to
decline slightly, from 1.8 per cent in 2015–16 to 1.5 per cent in 2018–19 as a
result of the Bill.[23]
2.13
The AMA submitted that they support the removal of the conscientious
exemption category as a measure to increase vaccination rates in children.[24]
The AMA also stated that preliminary data suggests that some conscientious
objectors may already be reconsidering their position because of the measures
proposed in the Bill.[25]
The Northern Rivers Vaccination Supporters told the committee that as a direct
result of the proposed legislation, vaccine-hesitant parents have approached
the group seeking more information about vaccination.[26]
2.14
DSS told the committee that allowing conscientious objection to
vaccinations is contradictory to its position that 'immunisation is an
important public health policy'.[27]
The Government has also stated that the policy will give confidence to parents
who vaccinate their children and send them to child care centres.[28]
Expanding eligibility range
2.15
The committee heard that this Bill would also further encourage
vaccination rates in all children by requiring that children are up to date
with their vaccinations each year until they turn 20.[29]
This will capture parents who receive Child Care Benefit and Child Care Rebate
for children aged eight to 20, some of which will be before-and after-school
care, and those receiving FTB-A supplement and who have not fully vaccinated
their children, whether or not they are registered as a CO.[30]
2.16
DSS provided the committee with a table of children expected to fail the
immunisation requirement to receive FTB-A supplement by year of age[31]:
|
|
2015-16
|
2016-17
|
2017-18
|
2018-19
|
|
Age 1*
|
3,100
|
2,800
|
2,500
|
2,100
|
|
Age 2*
|
3,200
|
2,900
|
2,500
|
2,200
|
|
Age 3
|
7,100
|
6,300
|
5,500
|
4,600
|
|
Age 4
|
7,200
|
6,400
|
5,500
|
4,600
|
|
Age 5*
|
3,200
|
2,900
|
2,500
|
2,200
|
|
Age 6
|
8,200
|
6,400
|
5,500
|
4,600
|
|
Age 7
|
8,100
|
6,500
|
5,500
|
4,600
|
|
Age 8
|
8,500
|
6,100
|
5,700
|
4,500
|
|
Age 9
|
9,400
|
6,500
|
5,500
|
4,900
|
|
Age
10
|
10,000
|
6,900
|
5,600
|
4,600
|
|
Age 11
|
14,600
|
7,700
|
6,400
|
5,100
|
|
Age 12
|
16,300
|
10,900
|
7,100
|
5,700
|
|
Age 13
|
14,800
|
12,300
|
10,100
|
6,300
|
|
Age 14
|
18,500
|
11,200
|
11,500
|
9,200
|
|
Age 15
|
23,200
|
13,600
|
10,200
|
10,200
|
|
Age 16
|
20,500
|
15,300
|
11,300
|
8,200
|
|
Age 17
|
20,200
|
12,400
|
11,600
|
8,300
|
|
Age 18
|
8,000
|
5,900
|
4,600
|
4,200
|
|
Age 19
|
400
|
300
|
300
|
200
|
|
Total
|
204,500
|
143,300
|
119,400
|
96,300
|
2.17
Some submitters were supportive of the expansion of the eligibility
requirements to be checked each year up to age 20.[32]
DSS told the committee that the majority of families who immunise their
children as a result of this Bill are expected to do so as a result of
eligibility being checked each year until age 20.[33]
Alternative measures to increase
vaccination rates
2.18
Submitters and witnesses suggested that the Government implement other
means of increasing vaccination rates, including addressing access issues, improving
education about vaccines and a national vaccine reminder system.[34]
Targeting unvaccinated children who
are not registered conscientious objectors
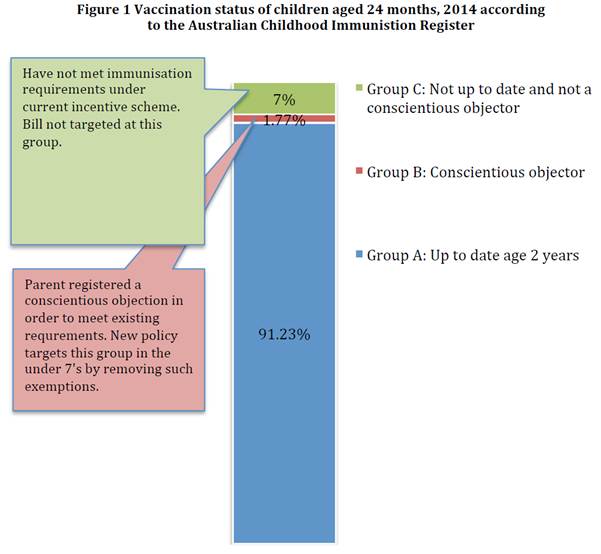
2.19
Submitters and witnesses presented the committee with evidence that COs
account for only a small portion of the total number of families who do not
vaccinate (See Figure 1). As noted in Figure 1, unvaccinated children who are
not registered as COs account for 7 per cent and COs account for 1.77 per cent
of all children under 24 months in 2014 according to the Australian Childhood
Immunisation Register (ACIR). Professor Leask submitted that these children are
not fully vaccinated for a range of reasons including: incorrect data in ACIR; they
are children of 'silent' unregistered objectors; and practical barriers to
vaccination. Professor Leask told the committee that neither the current
legislation that attaches vaccination to social security payments nor the
proposed Bill have or will influence this group.[35]
 Source: Submission 327, p. 2.
Source: Submission 327, p. 2.
2.20
The Public Health Association of Australia (PHAA) told the committee
that the Government should seek to address the structural and practical
barriers to vaccination that exist, including socioeconomic reasons that
children are not vaccinated.[36]
The Royal Australasian College of Physicians (RACP) suggested home visiting
programs would be one way of overcoming practical barriers to vaccination.[37]
Communication and education
strategies
2.21
Some submitters expressed concern that some immunisation providers do
not possess extensive knowledge on vaccinations.[38]
The PHAA told the committee this was crucial to successfully engage with
vaccine hesitant parents.[39]
Professor Leask suggested that the Government consider the value of increasing
vaccination training in the medical curriculum.[40]
2.22
Professor Leask also recommended that the Government investigate the
following strategies to reduce the incidence of vaccine refusal:
-
parent peer-advocate training in
regions with higher rates of vaccine refusal;
-
competitively awarded funding for
local community campaigns designed by and for each community;
-
inclusion of education about
vaccination in high school core curriculum; and
-
funds to support more access to
immunisation nurse accreditation training and better access to, and
incentivisation of, training and updates for midwives.[41]
2.23
Professor Leask suggested that Primary Health Networks could play a key
role in education and training about vaccinations at a community level.[42]
2.24
Evidence provided to the committee indicates that there is significant
confusion as to which vaccines are mandatory for eligibility. The committee
notes the different information provided on the each of DSS,[43]
the Department of Human Services (DHS)[44]
and the Department of Health (DoH)[45]
web sites. The committee notes that on the DHS website it states that 'most of
the immunisations on the National Immunisation Program Schedule are linked to
family assistance payments'.[46]
2.25
The committee notes that the Government has announced $26 million in
funding for Immunise Australia, as part of a 'balanced carrot and stick
approach'.[47]
The funding will include: incentive payments to immunisation providers who
identify under-vaccinated children and initiate a catch-up schedule; improving
public vaccination records and reminder systems; and communication strategies
to promote the benefits of vaccinations.[48]
2.26
The PHAA told the committee that implementing a successful reminder
system would have obstacles, as contact details for parents may be incorrect
due to the fact that vaccination providers are no longer able to update address
details of their patients in ACIR – parents have to contact DHS directly.[49]
2.27
DSS, the lead agency for this legislation, told the committee
communication activities are a joint responsibility of DoH, DHS, The Department
of Education and Training (DET) and DSS. DSS has been tasked with the following
communication activities:
-
child care centres will be sent an
e-kit via the Child Care Management System. It will include a printable PDF
poster the centres can display and immunisation specific text that they can
send out to all their families in newsletters and questions and answers;
-
Members of Parliament and Senators
will be sent a similar e-kit that will also include a shell release;
-
a social media campaign that
targets families with children under 20. The Facebook campaign will direct
families to the Department of Human Services website
www.humanservices.gov.au/immunisation, which is the key source of all
information relating to immunisation and No Jab No Pay measure;
-
the social media campaign will
complement the activities of the Department of Health, Department of Humans
Services and the Department of Education (noting that all families that do not
meet the immunisation requirements and receive child care payments will get a
letter from Centrelink before their payments are affected letting them know
what to do and when); and
-
additional communication
activities for early 2016 may be deployed as required to ensure the community
and stakeholders understand their obligations under the changes.[50]
2.28
The committee sought clarification on the detail of the Government's
education campaign for vaccination but has not been provided information on the
activities and budget of the other departments.
Impact on disadvantaged families
2.29
Submitters were concerned that the Bill unfairly and disproportionately
affects low-income families whilst simultaneously not addressing the barriers
to vaccination that may exist for families who are not opposed to vaccination.[51]
2.30
Submitters argued that the Bill is unfair because only wealthy families
could afford to exercise their objection to vaccinating their children.[52]
Children of conscientious objectors
2.31
Where the measures in the Bill are unable to persuade parents to
vaccinate, submitters and witnesses have raised concerns that this may lead to
further disadvantaging children of COs.[53]
2.32
Submitters argued that children should not be further disadvantaged by
the choices made by their parents.[54]
The Law Institute of Victoria's submission raised concern that the Bill may
have the unintended consequence of further disadvantaging the children of
parents who choose to forgo the social security benefits.[55]
2.33
Inspired Family Day Care Service is a national child care service
provider that does not support the Bill, argued that the Bill infringes on a
child’s right to education:
By refusing child care assistance to non–vaccinated,
partially vaccinated and conscientious objectors, the Commonwealth is
determining who may or may not attend child care, in particular further marginalising
at risk and low socio-economic families and creating a cycle of non-access for
educational engagement.[56]
2.34
However the committee also heard that in areas where vaccination rates
are well-below the national average, parents of young children are avoiding
mothers groups for fear of the risk posed by unvaccinated children. As a
result, those children are missing out on 'valuable social interactions' and
the parents are missing out on valuable support groups.[57]
The AMA told the committee that 'all children have the right to be protected
from vaccine preventable diseases' but urged the Government to monitor the
impacts of the Bill to ensure that children are not being increasingly
disadvantaged by reduced access to child care.[58]
2.35
The committee inquired into the analysis that DSS undertook into the
demographic of those affected by the Bill, such as their income levels and
geographic dispersion. DSS told the committee that they did not have sufficient
data to determine the income levels of COs or provide meaningful analysis of
the geographic dispersion of those affected by the Bill.[59]
Changes to the 63-day grace period
2.36
The National Welfare Rights Network told the committee that they were
concerned about the Bill's proposed changes to the 63-day grace period, whereby
under the proposed Bill, there is no grace period for children who are applying
for the first-time for child care payments. However, once the child commences a
catch-up schedule they are considered eligible for payments. National Welfare
Rights Network submitted that this potentially disadvantages these families who
may be new foster parents, adopted parents or grandparent guardians, if they
face a delay in visiting a general practitioner to commence a catch-up
schedule.[60]
Evaluation of the Bill's impact
2.37
Submitters suggested that the Government monitor the impact of the Bill
on vaccine hesitant families and vaccination rates.[61]
Professor Leask recommended a full evaluation of the policy's impact in
2018–19 on:
-
vaccine refusing families on low
incomes;
-
vaccine confidence;
-
immunisation providers and primary
care service delivery;
-
vaccination rates;
-
refusal rates;
-
child care arrangements of vaccine
refusers;
-
outbreaks; and
-
any other impacts.[62]
Suitability of proposed exemption categories
2.38
The committee heard concerns about the removal of conscientious
objection as an exemption category and issues about the medical exemption
category.
Removal of conscientious objection
category
2.39
Submissions to the inquiry indicated a range of reasons as to why people
conscientiously object to vaccination. These can be generally divided into four
broad categories:
-
concern for the safety and/or efficacy of vaccines;[63]
-
those who were unable to obtain a medical exemption where they
believe it is warranted;[64]
-
religious beliefs that are not recognised by the Government;[65]
and
-
ethical reasons such as the use of animal products.[66]
2.40
Many submitters states that conscientious objection is based on
considered personal beliefs and circumstances which inform people's decision not
to vaccinate their children.
Concern for safety and efficacy
2.41
Submissions expressed concern about the safety of vaccines and argued
that the Bill may put children at risk of injury by encouraging parents to
vaccinate.[67]
Other submitters told the committee that they hold concerns about the efficacy
of vaccines and the regulatory requirements necessary to have a vaccine
approved. As a result, some parents have chosen to partially vaccinate their
children while others have never vaccinated.[68]
2.42
Submitters and witnesses were particularly concerned about the safety of
administering multiple vaccines in a short period of time and called for
evidence that shows the safety of the national vaccine schedule as a whole.[69]
The AMA told the committee that 'the human body can cope with multiple antigens
being exposed all at the same time and develop quite good immunity without any
ill effects'.[70]
2.43
Some submitters claimed that Australia's immunisation schedule has more
vaccines that are given at a younger age than other developed nations, notably
Japan. Submitters and witnesses told the committee that Japan does not
vaccinate children under two years of age and have ceased the Human
papillomavirus (HPV) vaccine.[71]
However, evidence from the World Health Organisation that was provided to the
committee refutes these claims, showing that Japan's vaccine schedule does
include these types of vaccines.[72]
2.44
Submitters and witnesses were particularly concerned about the safety
and effectiveness of the pertussis (whooping cough) vaccine. The committee
heard a range of concerns about the vaccine that included:
-
the number of booster shots needed for effectiveness;
-
the accuracy of information about the seriousness of the disease;
-
adverse reactions to the vaccine;
-
that whooping cough is more prevalent today than in previous
years[73];
2.45
The AMA told the committee that the pertussis vaccine gives a high level
of protection but is not 100 per cent effective and is not lifelong; rather the
vaccine greatly enhances the immune system but the vaccinated person can still
catch the disease. Because of this, babies are targeted as early as possible
along with their families as an 'imperative'.[74]
2.46
The RACP told the committee that in older versions of the pertussis
vaccine, there were cases of children having a 'dramatic colour change', and
RACP noted that the newer vaccines do not produce this reaction.[75]
2.47
The committee sought information from DoH regarding the effectiveness
of the pertussis vaccine. DoH advised that information is publicly available
from the Pharmaceutical Benefits Advisory Committee.[76]
2.48
Many submitters raised concerns about the safety of vaccines that are
not mandatory for eligibility of social security payments. Of particular
concern were the Hepatitis B vaccine given at birth[77]
and the HPV vaccine to 10 to 15 year olds.[78]
Hepatitis B is a mandatory vaccination for babies at two months, four months
and either six or 12 months but is not mandatory for newborns.[79]
The RACP told the committee that the Hepatitis B vaccine is recommended in
physiologically stable babies and that it is not offered to very premature
babies.[80]
RACP told the committee that the HPV vaccine is very safe and they have no
concerns.[81]
2.49
In a written question on notice to DoH on 5 November, the committee
sought clarification of the information that the Department of Health provides
on its website about the Hepatitis vaccine. A response had not been received at
the time of tabling.
2.50
Submitters and witnesses told the committee that the true number of
adverse reactions to vaccines was much higher than reported.[82]
One submitter referred the committee to a media release by the Therapeutic
Goods Administration in 2014 that says:
It is generally acknowledged that adverse events [for
medicines and vaccines] are under-reported around the world, with estimates
that 90-95% of adverse events are not reported to regulators.[83]
2.51
The AMA told the committee that depending on the severity you are
considering, the risk of a severe reaction to a vaccine can be somewhere
between one in a million and one in 100,000.[84]
2.52
DoH told the committee that serious adverse events are recorded by the
Therapeutic Goods Administration. DoH said that in 2014–15 of the 10.8 million
doses administered under the National Immunisation Program, there were 243
serious adverse events reported or 0.002 per cent.[85]
Medical exemption category
2.53
Submitters told the committee that as the Bill proposes to remove
conscientious exemption, there needs to be greater scrutiny of what they
perceive to be the narrowness of the medical exemption category. The committee
heard that some people are COs because they are unable to receive a medical
exemption for their child where they believe it is warranted. This group tend
to believe that vaccines are safe and effective, but that their own child falls
into the small percentage of children who suffer adverse events that should
warrant a medical exemption.[86]
2.54
Submitters expressed concern about the restrictiveness of receiving a
medical exemption for their child and also indicated that doctors can be
reluctant to give medical exemptions in some situations.[87]
Submitters told the committee reasons they as parents or guardians had sought
medical exemption but were denied included:
-
the child had a severe reaction to a different vaccine;[88]
-
the child's siblings severely reacted to certain vaccines;[89]
and
-
a family history of severe reactions to vaccines.[90]
2.55
Under the proposed Bill, medical exemptions can be approved by a general
practitioner. The committee notes that currently medical exemption can be approved
by a medical practitioner for the following medical contraindications:
-
unstable neurological disease;
-
encephalopathy within 7 days after
a previous vaccination;
-
immediate severe acute allergic or
anaphylactic reaction after any previous vaccination;
-
malignant disease and/or
immunosuppressive therapy and/or immune suppression; and
-
allergy to preservative or
antibiotic contained in the vaccines;
-
OR
-
the child has other non-permanent
contraindication and vaccination is deferred.[91]
2.56
In regards to a family history of severe reaction to vaccines, the AMA
told the committee that 'anaphylactic reactions tend to be one-off',
idiosyncratic and do not generally run in families.[92]
2.57
The AMA told the committee:
The AMA recognises that the Australian Immunisation Handbook
(currently 10th Edition, updated in June 2015) a key document in terms of
providing guidance to GPs [General Practitioners] about exemptions to
immunisation. Contrary to what the earlier witnesses indicated, the Handbook
provides information on a range of contraindications and precautions that need
to be taken with certain groups such as those who are at risk of anaphylaxis,
those who are immunocompromised, those who are receiving immunoglobulin or
other blood products etc. This material is contained in sections 4.9.9
Contraindications and 4.9.10 Precautions. Further material on at risk groups
or possible exemptions is also provided under each listed individual disease
names.
It is also critical to recognise that GPs will also use their
clinical judgement in assessing children who are eligible for a medical
exemption. As Dr Kidd testified, medical exemptions are rare, but with the
guidance provided by the Immunisation Handbook, and their own clinical
judgement, GPs are well equipped to identify the small number of children who
should not receive vaccination.[93]
2.58
DoH told the committee that they are looking to strengthen and clarify
to vaccine providers and the broader community what is an acceptable medical
exemption including what types of allergic reactions warrant a medical
exemption.[94]
Part of this process includes consulting with the General Practitioner
Roundtable, National Immunisation Committee and DHS.[95]
2.59
The committee sought further explanation about the types of medical
contraindications that warrant a medical exemption from DoH. A response had not
been received at the time of tabling.
Allegations of coercion
2.60
Submitters expressed the view that the significant loss of financial
benefits, particularly for low-income families who are COs, would be tantamount
to removing the choice of parents to give free, informed consent to the vaccination
of their children.[96]
Submitters referred to the Australian Immunisation Handbook that states that
vaccinations must only be administered 'in the absence of undue pressure,
coercion or manipulation'.[97]
Submitters also suggested that the proposed measure contravened a number of
human rights conventions, including the Universal Declaration of Bioethics and
Human Rights and the International Covenant on Civil and Political Rights
(ICCPR).[98]
2.61
Article 6 of
the Universal Declaration of Bioethics and Human Rights states:
Any preventive, diagnostic and therapeutic medical
intervention is only to be carried out with the prior, free and informed
consent of the person concerned, based on adequate information. The consent
should, where appropriate, be express and may be withdrawn by the person
concerned at any time and for any reason without disadvantage or prejudice.[99]
2.62
The Parliamentary Joint Committee on Human Rights (PJCHR) found the Bill
engages and places limits on the right to freedom of thought, conscience and
religion as set out in article 18 of the ICCPR and has sought advice from the Minister
on whether the measures are justifiable.[100]
2.63
The AMA submitted that some parents will continue to hold strong views
against vaccination but that they will continue to have the choice to
vaccinate.[101]
DSS submitted that the limitation of some rights is 'necessary and
proportionate to the legitimate aim of promoting the right to physical and
mental health'.[102]
In regards to article 18 of the ICCPR, DSS said:
...these freedoms may be subject to limitations as prescribed
by law and which are necessary to protect public health or the fundamental
freedoms of others. The objection to vaccination can limit the rights of others
to physical and mental health. As the most effective method of preventing
infectious diseases, vaccination provides a necessary protection of public
health.
Further, these families continue to have the right to uphold
their conscientious or religious belief by electing not to receive child care
benefit, child care rebate or the family tax benefit Part A supplement.[103]
Vaccination injury compensation scheme
2.64
Submitters and witnesses suggested that Australia establish a vaccination
injury compensation scheme.[104]
The RACP advocate for the introduction of a compensation scheme and provided
the committee with the following statement:
Since immunisation benefits the population as well as the
individual, it is entirely just and reasonable that society as a whole accepts
vaccine damage compensation for affected individuals and their families. This
has long been the case in New Zealand; it is yet to be accepted in Australia.
The RACP strongly supports introduction of an Australian no fault vaccine
compensation scheme, either as part of a national disability scheme or injury
insurance scheme, or separately.[105]
2.65
Submitters and witnesses argued that because vaccinations carry a small
risk of serious adverse reaction the Government should compensate the small
number of individuals who experience a severe adverse reaction in the interests
of protecting the broader community.[106]
Furthermore, some submitters argued that the Bill coerces parents to vaccinate
and therefore it is an ethical necessity to provide an accompanying vaccine
compensation scheme.[107]
2.66
The World Health Organisation reports that 19 countries currently have a
vaccine compensation scheme and considers them 'an important component for
successful vaccination programs'.[108]
Impact on child care providers
2.67
Childcare Alliance Australia told the committee that they sought
reassurance from the Government that child care providers will not be
financially impacted by the Bill, particularly during the transition phase.[109]
2.68
DET told the committee that 'consultation with the child care sector and
families was undertaken by DSS during June and July 2015.[110]
DET also informed the committee that they will distribute information about the
Bill 'directly to child care providers when the Bill passes the Senate'.[111]
DET further said:
...there is not expected to be a lengthy delay in approval of
an individual’s eligibility for Child Care Benefit and a child care service’s
ability to claim that payment on behalf of the family when the child commences
child care. In the interim, the child care service can charge the family the
full fee.[112]
Accuracy of the Australian Childhood Immunisation Register data
2.69
Submitters and witnesses expressed concerns about the accuracy of data
in the ACIR as well as the capacity to continue to monitor COs if the Bill is
passed.
Inaccurate records
2.70
A number of submitters and witnesses raised concerns that not all the vaccines
a child has received have been recorded properly in ACIR, resulting in fully
vaccinated children being recorded as ineligible for social security payments.[113]
2.71
Associate Professor Julie Leask told the committee she has been involved
in research that suggested that an estimate of between '18 per cent and 50 per
cent of those who are shown as not up to date on the register might actually be
up to date.'[114]
The submission from NSW Health noted this can occur due to data transfer errors
or from the fact that prior to 2015, 'vaccines given after seven years of age,
including those in high school programs, were not able to be recorded on the [ACIR].'[115]
Associate Professor Leask told the committee the issue this creates is that
some children received catch-up vaccines after the age of seven and therefore
they are not recorded.[116]
2.72
PHAA said that targeted data cleansing has been undertaken by divisions
of general practice, Medicare Locals and primary health networks which has
revealed a number of inaccuracies. PHAA told the committee of one example
recently in South Australia:
...a total of 886 Aboriginal children aged under seven years
were identified on ACIR reports as not fully immunised. After an extensive data
cleaning exercise was undertaken, 395 records were corrected, resulting in
children confirmed as fully immunised. With this proposed policy, these
families would have been financially penalised not because their child was not
fully immunised but because of a flawed database.[117]
2.73
Submitters and witnesses referred the committee to a recent report by
the Australian National Audit Office (ANAO). In June 2015 the ANAO released a
report into the audit of the administration of the ACIR. The report said that
while overall the DHS' administration of ACIR has been 'generally effective',
there 'remains scope to strengthen ACIR quality and control framework' and that
'maintaining ACIR data quality remains an ongoing business risk for the
department'.[118]
ANAO recommended:
To contribute to ACIR data integrity and improve the
efficiency of information processing, Human Services should establish a pathway
for the resolution of persistent and known data synchronisation issues between
ACIR and other departmental ICT systems, incorporating a planned process and
timetable. There would also be benefit in the department working with PMS
suppliers to identify options for addressing errors arising during data
exchanges between the ACIR and provider systems.[119]
2.74
ANAO also reported that while DHS relies on providers and parents to
assist in maintaining the accuracy of ACIR, DHS has not clearly and
consistently 'communicated its expectations on the key role played by parents
and immunisation providers'.[120]
2.75
The committee notes that the Bill proposes to increase the age and
frequency that eligibility for social security payments is checked. PHAA expressed
concern that 'the current structures in place to record immunisation would
struggle to cope with the expanded requirements that the Bill will place on
it'.[121]
Furthermore, PHAA told the committee that inaccurate data can lead to children
having unnecessary vaccines that are a wasted cost and a painful experience for
the child.[122]
PHAA told the committee ACIR was 'in urgent need of an upgrade'.[123]
Associate Professor Leask recommended a delayed start to the Bill to enable the
required changes to be put in place.[124]
2.76
DoH assured the committee that the Government is aware of the concerns
raised about data accuracy and that as part of the rollout of the Australian
Immunisation Register will be providing additional support to assist with 'data
cleansing', that is, to make the data more accurate. DoH is also investigating
the interaction between vaccine providers' software and DHS to improve the
accuracy of data collection.[125]
2.77
DHS notified the committee that in response to the ANAO report, DHS have
developed a Quality Strategy Plan, and they expect the actions of the plan will
be implemented before 1 January 2016.[126]
DHS further provided the committee with the following response about how it
intends to improve the accuracy of ACIR:
In accordance with the phased expansion of the Australian
Childhood Immunisation Register (ACIR) into a Whole of Life Australian
Immunisation Register (AIR), a range of improvements will be implemented to the
Register’s functions and operations. This includes new functionality to enable
providers to correct errors online through the AIR secure site, such as
correction of an incorrect dose number or incorrect vaccine recorded. This will
begin to be implemented in September 2017.[127]
2.78
Professor Leask recommended that the Government undertake a 'full review
of the implementation issues in 2017 with subsequent amendments to legislation
as needed'.[128]
Monitoring conscientious objection
2.79
Submitters and witnesses were concerned that the Bill will effectively
mean that COs will not be recorded on ACIR and therefore not recorded by the
Government.[129]
PHAA told the committee this information is important for policymakers when
planning communication strategies.[130]
Associate Professor Leask added that monitoring COs is important to 'detect
early warnings of a dip in confidence and address that at local levels'.[131]
2.80
Furthermore, Associate Professor Leask said in her submission that state
and territory governments have relied on the ACIR records of COs when applying COs
exemption to state and territory legislation regarding access to child care
centres. Submitters and witnesses suggested that the Government finds an
alternative means of counting conscientious objection.[132]
Committee view
2.81
The committee notes that vaccination is a highly emotive issue. The
committee wishes to reaffirm that the role of the committee is to consider and
report on the evidence provided that engages with the proposed legislation and
related policy issues. The committee does not make its considerations based on
the number of submissions received, but on considerations of the concerns
raised. The committee reaffirms that all issues raised in submissions and
correspondence received by the committee have been considered.
2.82
The committee notes that there is confusion about what vaccinations are
required for a child to be considered eligible for social security payments.
The committee suggests that the departments work together to create clearer and
more coherent communication about immunisation requirements.
2.83
The committee acknowledges that education and communication play a key
role in reducing vaccination refusal rates and increasing vaccination rates.
The committee notes the Government's budget commitment to communication
strategies and encourages the Government to consider the
strategies proposed by submitters to this inquiry.
2.84
The committee acknowledges concerns raised by the PJCHR and submitters,
that the Bill risks infringing upon the human rights of parents making
decisions about their children's health and the rights of children to access
child care services and early childhood education. However, the committee is
satisfied that these infringements are necessary and fairly outweighed by the
rights of all members of the community to health and that vaccination is a
critical and important health measure. However, the committee suggests that the
Government monitor the impact of the Bill on disadvantaged families.
2.85
The committee notes the concerns raised by submitters and witnesses of possible
unintended consequences of the Bill and considers that there is merit in
conducting an initial review after 12 months to assess the immediate impact of
the Bill and an evaluation of the impact and effectiveness of the Bill after
three years of implementation.
2.86
The committee expects that DHS will meet their target of implementing
the plan developed in response to the ANAO report and that DHS should examine a
means of monitoring conscientious objection in the community. The committee
considers these issues should be addressed prior to the implementation of the
Bill.
2.87
The committee acknowledges that vaccination carries a small risk of
severe adverse reactions. The committee recognises that Australia, unlike other
developed countries, does not have a national vaccine injury compensation
scheme and encourages the Government to examine the merits of such a scheme.
Recommendation 1
2.88
The committee recommends that the Government consider an initial review
after 12 months to assess the immediate impact of the Bill and a full
evaluation of the impact and effectiveness of the Bill after three years of
implementation.
Recommendation 2
2.89
The committee recommends that the Government consider the educational
and communication strategies to improve vaccination rates proposed by
submitters to this inquiry.
Recommendation 3
2.90
The committee recommends that the Government investigate a means of
continuing to monitor conscientious objection if the Bill is passed.
Recommendation 4
2.91
The committee encourages the Government to investigate the merits of a
national vaccine compensation scheme.
Recommendation 5
2.92
The committee recommends that the Bill be passed.
Senator Zed Seselja
Chair
Navigation: Previous Page | Contents | Next Page